Learning Objectives
This is an intermediate-level course.
After completing this course, you will be able to:
- Define and
describe transference as both a therapeutic construct and a therapeutic
process.
- Define and
describe countertransference as both a therapeutic construct and a
therapeutic process.
- Explain how archetypes trigger transference and countertransference during non-analytic therapy.
- Describe how therapists are likely to contribute to transference and countertransference phenomena.
This course is based on the most accurate
information available to the author at the time of writing. Cognitive
psychology and neuroscience findings regarding brain development, structures,
and activities continue to shed light on what were once regarded as merely
psychoanalytic concepts and processes. As a consequence, new information may
emerge that supersedes some explanations in this course.
This course may provoke disturbing
feelings in readers due to their own unresolved conflicts, but it also gives
them information about processes by which they might resolve these conflicts.
Outline
- Introduction
- Contemporary Environments and Neuroscientific Advances
- Language, Cultural Diversity, and Context
- The Phenomenon Called Transference
- Transference: Classical Definition
- Transference: Totalistic Definition
- A Description of Transference for Non-Analysts
- The Phenomenon Called Countertransference
- Countertransference: Classical Definition
- Countertransference: Totalistic Definition
- Descriptors of Countertransference
- A Definition of Countertransference for Non-Psychoanalysts
- Triggers of Transference and Countertransference
- Archetypal Material Is Embedded in Culture
- Final Thoughts
- Footnotes
- References
Introduction
Transference and countertransference are mental processes that enable us to move the past to the present and one
setting to another. We do so unconsciously. Sometimes we benefit from this
displacement, though usually only temporarily. But most of the time, sooner or later, we create problems in our lives and those with whom we interact because, in spite of their similarities, the past is not the present and one setting is not another.
We might think that these two unconscious processes will not interfere with our therapeutic efforts because we are not psychoanalysts. Transference? No. We help clients restructure the thoughts that they articulate. We help them manage feelings as they arise. We help them change behaviors. We focus on conscious processes. Countertransference? No. Before, during, and after sessions, we deal with personal issues that become apparent to us as well as to others.
Unfortunately, these presumptions are erroneous because transference and countertransference occur outside the realm of consciousness. They take place in session after session without our knowing it, whether we are trained to deal with them or not. Furthermore, they are potent, pervasive, and ubiquitous. Thus they have the potential either to make our work extremely helpful to our clients or to diminish – even prevent – the good we hope to do.
Hence the wisdom of our becoming aware of phenomena going on beneath the surface of our work, followed by our using them in such a way that they become benevolent mediators and moderators of positive therapeutic outcome. They are ever-present double-edged swords we can familiarize ourselves with by using respected psychoanalytic and psychodynamic theory and research to become proficient in transference and countertransference phenomena.
Now for a theoretical, research-based
overview.
Residing deep within the unconscious mind where there is no time (Freud, 1917), transference and countertransference become activated when similarities between the then-and-now as well as the here-and-there arise. Already encoded in subcortical neural pathways, material from our unconscious mind is propelled into our conscious mind as we try to reduce the pain of psychological phenomena we are experiencing. With the “help” of brain activity, we unconsciously revive and re-enact conflict-ridden experiences as if the past were the present and one setting were another. We transfer thoughts, feelings, and attitudes about people who resemble others. We assign them roles once played by others. We take on old roles ourselves. All unconsciously.
Why do we do this? For at least two reasons.
One is that we experienced conflicts in the past and/or in a particular setting. They were intrapersonal, interpersonal, or both. Those we could resolve, we did. Those we could not, remain. All conflicts are painful. Unresolved conflicts are doubly painful.
Because we benefit from getting get rid of pain, our brain has been evolutionarily programmed to try to resolve conflict by repeating or re-enacting it. It has unconsciously “concluded” that these methods will work, sooner or later.
In other words, we will be better off once a new experience replaces memories of a past event or another happening in another setting. For example, if our relationship with our mother was conflictual because she was abusive though she should have been loving, we assign a maternal role to our spouse and a child role to ourselves. We hope, indeed unconsciously believe, that in this re-enactment our spouse will treat us more lovingly than our biological mother did. Our conflict will be resolved and our pain replaced by well-being.
A second reason is that we live in fear – indeed terror – of some things that happened early in our life, starting in utero and with our birth. One example would be a death that we witnessed. Our little goldfish or our loving grandparents died. They shouldn’t have, but they did.
Thus we are left with a painful conflict: What we do not want to happen, happens. We do not have the power to stop it. We want the power and believe we should have it, but we don’t.
We find, however, that we can lessen our emotional pain by projecting it: transferring it from inside us to outside us. We give our parents power over death, for example, by listening carefully to them when they tell us to watch out for traffic before crossing the street lest we get killed. Then we “prove” it by obeying them. By crossing the street the way they say we should, we enjoy the illusion that death has no power over us. We get much-needed relief. That’s the good news.
The bad news is that we do not actually resolve our conflict over wanting to prevent death and being powerlessness over it. So we try again and again to gain that power through the transference process.
In other words, initially transference does solve our problem. It is a “creative projection” (Becker, 1973, 158) of something inside us to someone outside us. It serves an adaptive response to our need to empower ourselves. It allows us to survive with the help of others. We can transfer our terror of the inevitability of death – over which we are powerless – to others. As Becker (1973) explains, transference is an illusion, but a “life-enhancing illusion” (158) that brings us relief. Indeed, transference is actually necessary for our psychological well-being at the time we use it. It is the benevolent edge of a double-edged sword.
The malevolent edge? Our relief is only temporary. Others will inevitably fail to live up to our expectations that they can prevent death from happening. Death will occur, whereupon our emotional pain will be resurrected. Our well-being will give way to the pain inherent in our original conflict: wanting to prevent death, but not being able to do so.
At the same time, because we benefit from transference, we continue to use it. Even though temporary, our getting relief serves as a positive reinforcement. We have been programmed through operant conditioning to repeat the process. Again and again and again. It will become a compulsion, as noted by Freud (1912) more than a century ago.
In sum, though transference does not effectively resolve conflict, we unconsciously continue to use it. What we actually need to do, however, is learn to resolve our conflict by facing it squarely, experiencing the pain of our powerlessness, and accepting it as part of the human condition. In other words, we need to deal with transference on a conscious level. We need to undermine its influence over our unconscious mind. Indeed, we need to turn it back on itself and thus benefit from it.
In sum, we need to do what is actually possible for us: outwit the double-edged sword we call transference and its counterpart, countertransference. We need to take control over transference and countertransference, for they are the worst of masters but the best of servants (Davids, 2022).
Hence, this course:
- A course for non-analytic psychotherapists whose work is being significantly influenced by transference and countertransference although they specialize in dealing with conscious phenomena;
- A course that exposes the dangers of not undermining brain activity that imposes old schemas on new experiences simply because of similarities;
- A course that outlines how to stop displaced phenomena from running rampant during the course of psychotherapy; and
- A course that spells out how to benefit from resolving conflict, embracing the pain inherent in it, mourning what ideally should not have happened to us, and moving on.
This is the first course in a three-part
series, based on the book Transference and
Countertransference in Non-Analytic Therapy: Double-Edged Swords,
by Judith A. Schaeffer, Ph.D. (Lanham, MD: University Press of America, 2007).
(Note: To return to the course after clicking a footnote, click the Back button in your browser.)
Contemporary Environments and Neuroscientific Advances
Three developments make this course
especially pertinent for today’s mental health professionals.
First, 21st century clinicians
no longer have the option of open-ended treatment, even for dealing with
serious disorders, because of managed care’s concerns about cost-effectiveness.
They must identify and manage impediments to progress as soon as they arise so
that clients finish their work within their allotted sessions. Thus they must bring unconscious impediments to reaching their goals to the light of consciousness. In other words, treatment referred to as psychotherapy is to be a stage on which therapists help clients work “through the past and work toward the future” (Atlas, Aron, & 2018, p. 5). It is a “joint rehearsal on a stage…,” “an opportunity for” things to change “offstage” also (Atlas & Aron, 2018, p. 5).
In addition, most managed care companies require clinicians to translate outcomes into observable new behaviors and diminished, if not eradicated, symptoms. Clinicians must define what they do by functions that measure change. They must be aware of all variables that determine whether that change occurs. Thus they must know how transference and countertransference impact goal attainment.
Second, clients and their families expect
timely, ethical, and efficacious treatment. They belong to a litigious society
eager to right wrongs. Though serious errors may be rare, unaddressed
transferential and countertransferential material can result in mistakes which
clients or their families can bring to the attention of grievance boards or
lawyers. Should clients complete suicide, for example, their survivors may hold
the professionals who treated them responsible for not picking up transferential
signs of suicidal intentions.
Third, recent cognitive and neuroscientific research findings have revealed that transference and countertransference are actually instantiated in the brain (Anderson and Przybylinski, 2012; Shore, 2021; Pally, 2001; Gabbard, 2001). It is no longer scientific to deny their existence and activity in psychotherapy, no matter what a clinician’s theoretical orientation.
In other words, transference and countertransference propel conflictual unconscious material into the dynamics of both analytic and non-analytic therapy. If non-analytically oriented therapists fail to notice these displaced phenomena during their sessions, they are limited in their ability to help their clients move beyond their one-sided accounts of problematic relationships and events outside of therapy. Contrastingly, if they identify and decode that material during sessions, therapists’ perception of what is going on relationally in therapy can complement, if not correct, clients’ accounts of what happens to them outside of therapy.
As a result, clients can realize that what
is transpiring in therapy is similar to the unresolved conflicts at the core of
their presenting problems. This, in turn, can lead to conflict resolution.
Simultaneously, therapists can realize
how, through countertransference, they are also acting out old, conflictual
interpersonal issues in their relationship with clients. Then they, too, can
choose conflict resolution over mindless repetition.
In sum, "the future of psychotherapy … lies with the further development of short-term therapeutic techniques" that reduce the length of treatment while dealing "economically and effectively with the deluge of emotional and behavioral problems" that our disturbed society has spawned (Marmor, 1989, 259). Adding a focus on transference and countertransference enhances non-analytic clinicians’ otherwise efficacious work. For they are often the greatest hope for transformation in psychotherapy (Davies & Frawley,1992).
Language, Cultural Diversity, and Context
In this course, jargon is replaced by commonly used terms for the sake of readers not versed in psychoanalytic terminology. In addition, efforts are made to identify common culturally-based expectancies therapists and clients bring to their interactions. Finally, select aspects of analytic theories are placed within the context of non-analytic theories so that readers can integrate new material with what they already know.
The Phenomenon Called Transference
We all engage in transference. It is a pervasive and ubiquitous phenomenon that takes place in many situations in life (Brenner, 1982). It “occur[s] in virtually all close relationships” (Gelso & Bhatia, 2012, 384). Indeed, along with countertransference, it is “an inevitable part of relationships,” (Egan, 2022, 19). We re-experience the past in the present in a way that is inappropriate for the present (Greenson & Wexler, 1969). We misperceive or misinterpret the present in terms of the past.
We unconsciously send the “message” to select persons currently in our life that they have replaced significant others in our past. We impose what took place in one setting on what is taking place in another because in the previous one we could not resolve a conflict. We displace what still warrants our attention because it distresses us.
We will focus on the clinical setting because positive therapeutic outcomes depend on proper management of transference in non-psychoanalytic, no less than psychoanalytic, therapy (Gelso & Bhatia, 2012). Moreover, within the clinical setting, transference becomes concentrated, pronounced, and intense (Wilson & Weinstein, 1996).
Note that in this course, in keeping with psychoanalytic tradition, transference is attributed to clients and countertransference to therapists. In fact, however, both clients and therapists engage in transference and countertransference.
We’ll start with transference.
It is challenging to define transference because the term has been used inconsistently and ambiguously since Freud’s use of it at the dawn of the 20th century. Its precise meaning has never been agreed upon.
Thus, we will first focus on how transference has been described and defined in representative literature. Then we will create a theoretical definition that distills the essence of transference from its complexity. Finally, we will formulate an operational definition usable in clinical practice.
Transference: Classical Definition
Freud’s (1917) description of transference
serves as a prototypical classical definition of both a construct and a
process. As a construct, transference is clients’ displaced, early-life,
unresolved conflictual feelings and attitudes that surface in response to
experiencing their therapist. Transference is a matter of displaced memories of
affective and somatic states related to early-life significant others. It is a
matter of memories recalled by clients when they engage in therapy in such a
way that they are indistinguishable from events that occurred in the past
outside of therapy. “Transference is … the manifestation of unconscious …
memory as it intrudes upon the larger consciousness of self, breaking it up,
stunting it, and even at times, taking it over entirely” (Meares et al, 2005,
290).
As a process, transference is clients’
unconscious displacement of feelings, attitudes, sensations, and thoughts about
or toward persons in their early life to their therapist. Almost always, clients
do so because they could not resolve conflicts with those early persons. Instead,
they repressed them, burying them deep in the unconscious mind. Thus Freud
(1917) sees transference as serving the purpose of giving clients “new editions
of old conflicts” (454) so that they can resolve them. In other words,
transference is clients’ making an early-life event reappear in their
unconscious minds, an event from which they had to quickly dissociate because
of its overwhelming emotional impact (Schore, 2003a).
Lear (1993) calls transference an
unconscious movement of conflictual desire and/or belief across space and time
from one person in the past to another person in the present. It provides
another chance for clients to face psychic pain long enough and well enough to
resolve the conflict that caused the pain in the first place (Freud, 1917).
Interestingly, the unconscious mind prefers to avoid direct conflict resolution. It wants conflict to be resolved indirectly. Thus a problem: avoidance is reinforcing because it provides temporary relief from psychic pain. In time, the pain resurfaces, and transference has to be employed again. Thus conflicts never get the direct attention they need to be resolved. Another problem is that over time, this takes a significant toll on the psyche.
Pierro and colleagues’ (2008) research reveals new, useful data. The unconscious mind wants closure after gathering painful information. But particularly if it is a strong “J” on the Myers-Briggs scale, it wants closure as soon as possible. Thus people with a “J” preference (Judging) over “P” (Perceiving) are especially vulnerable to using transference as a means of avoiding conflict resolution. A reasonable deduction is that this becomes the case for “P”-preference people also because of ever-increasing distress when conflict remains unresolved (Ecker & Hulley, 1996).
At the same time, transference should be appreciated for what it does. The relief it provides at the time it is done is desirable, even necessary, for functioning, explains Becker (1973). It is an adaptive response to our awareness that we need a connection to others to cope with what life brings us. It is not possible to do so individually. In particular, we cannot stop death from happening, but we can cope with its inevitability by transferring our terror of death and our need to have power over it to another person. In other words, transference does solve a problem. It is a “creative projection” (Becker, 1973, 158). It is an illusion, but a “life-enhancing illusion” (158).
Transference as Involving Projection and Introjection
In the therapeutic setting, transference is
the projection of some aspects of a figure in the client’s past onto the
therapist. For example, as clients displace their fear of their critical mother
to their therapist, they attribute to their therapist their mother’s habit of
criticizing them. “You are like my mother,” the client senses, “and like my
mother, you will criticize what I do. I am no more powerful to stop you
than I could stop her. But I can at least placate you by doing the homework you
assign.” Another example would be Caucasian clients unconsciously projecting their own undesirable and unacceptable qualities on racial-minority therapists and making Whiteness a standard against which therapists are evaluated (Tummala-Narra, 2019).
As clients engage in projection, therapists engage in introjection. They unconsciously receive what clients send. “You perceive me as your critical mother and believe I will criticize you,” therapists sense. Then they tell themselves, “I can do nothing to prevent you from fearing my criticism, but I can come to your assistance by overlooking that you did not do the homework.” Or racial minority therapists whose countertransference mirrors their clients’ transference unconsciously tell themselves, “I must be exceedingly careful to come across as having the mannerisms of White people.” Ironically, noticing this subtle effort, clients then tend to confirm their belief that their therapists are indeed not White. They might even unconsciously conclude that their own inferior work, as non-White persons, is the reason they are not making progress.
It is of utmost importance to note that therapists engaging in introjection receive projections without identifying with them or owning them and the feelings connected with them (Stamm, 1995). They “accept” projections without necessarily confirming the perceptions inherent in them (Schafer, 1968).
Rather, therapists’ confirmation of a projection depends primarily on their own countertransference: displacement of their own unresolved conflicts (Westen & Gabbard, 2002). It depends on “the extent to which the [client’s] projection meshes with aspects of the therapists’ unresolved … conflicts ….” (Meissner, 1996, 43). Some therapists, for example, have not resolved their own conflict over mothers being critical of their children although they should accept them unconditionally. It is likely that their own mothers were routinely critical and, as a consequence, they hold templates of mothers as critical. Thus they unintentionally confirm their clients’ projection of them as critical. Consequently, they engage in some form of fault-finding. They routinely bring their clients’ attention to being slightly late, for example.
On the other hand, therapists who have resolved their own conflict over mothers being critical are not likely to confirm a projection of them as critical. They do not find fault with clients who send them projections of their being critical. They do not ordinarily call clients’ attention to being slightly late. Or they ask to explore with them client why they did not do their homework. They come across to their clients as respectful and/or curious rather than critical. 1
It is also important to keep in mind that clients who project do not recognize what they project as their own. It feels foreign to them. Something that they dislike seems to be coming at them, but it is not
theirs. They can sit back and criticize their therapist for what appears to be his or her negative trait or habit, oblivious to the fact that they are finding fault with themselves and thus projecting that unwanted trait. Hence, though the authors of the DSM-5-TR do not address transference directly, they do classify projection as a defense mechanism that is “almost invariably maladaptive” (Kupfer et al, 2013, 819; American Psychiatric Association, 2013).
Transference as Unconscious
Freud (1912) insisted that transference be regarded as fundamentally unconscious. Though clients may become aware of something calling forth their transference, they are not conscious of the relationship between that present stimulus and a past phenomenon. Their feelings about their therapist, for example, seem reality-based in the here-and-now.
Thus transference has been described as unconscious “meta-language” that carries meaning from clients to therapists.
As neuroscientist Schore (2003a) explains, the right hemisphere of clients communicates emotional states in nonverbal ways to the right hemisphere of therapists. Operating on a symbolic dimension (Lacan (1966), it uses symbols to convey information to the conscious mind (Epstein, 2023). 2
Thus, for instance, therapists receive the message on some instinctual, subliminal level that they have become their clients’ mother figure, for example, and that their clients feel toward them the same way they felt toward their actual mother. Therapists might later recall a gesture or posture of clients that probably served as a stimulus for their awareness, but at the time they were not conscious of that stimulus. Their clients simply and mysteriously sent a message which they simply and mysteriously received.
As an unconscious process, transference is no more accessible to clients’ conscious mind than other unconscious processes. While they may become distressed by bodily sensations, fantasies, dreams, and other manifestations of transference, they do not connect their distress with transferred material. As a result, they either move on to an issue of which they are conscious, or attribute their distress to a non-displaced, purely here-and-now phenomenon. Clients who transfer to therapists their fear of a critical mother, for example, might experience cold, metallic sensations. They might unwittingly assume postures indicative of avoidance as they project a negative maternal role onto their therapist. But, if they try to find an explanation for what they feel or do, they simply attribute what is going on to their therapist’s negative ways.
Without learning new skills, they are not able to access the material they have displaced. However, with these skills, they can process displaced material and thus prevent a maladaptive behavioral response to a transferential experience. Transference itself, along with an unconscious reaction to it, cannot be prevented, Anderson and Przybylinski (2012) emphasize. But after picking up cues or manifestations of transference, clients can choose adaptive behavioral responses to transferred material. To use Anderson and Przybylinski’s (2012) excellent recommendation, therapists can help clients design and install an if-then schema that they can then quickly engage. “If this happens, then I will say/do this” can guide their behavior, be it verbal or non-verbal. Thus in time, they will form the habit of responding differently after their initial reaction.
Transference as Fantasizing
Without such an intervention, most clients will rarely subject transferential material to reality testing. They will not use their conscious mind to distinguish facts from fantasy. If their conscious mind does anything, it will disregard the displaced material as an illusion unworthy of further attention.
Thus transference is a form of unconscious fantasizing that requires the reality-testing left hemisphere, or left brain, to be held in abeyance (Herron & Rouslin, 1982). Transference occurs naturally because the right-brain-to-right-brain communication at the heart of transference by and large prevents the left brain from acting.
Consequently, the transference process involves erroneous perception and extremely simplified cognition that work together to distort reality. Furthermore, this activity of the right brain occurs immediately and effortlessly upon cues of similarity being detected (Anderson & Przybylinski, 2012). One or two similarities are recognized, while many dissimilarities are dismissed. Clients simply fantasize, for example, that their therapist is another critical person with whom they have had a conflictual relationship. They do not take time to evaluate whether that fantasy matches reality or is a figment of their imagination.3 Indeed, it usually does not even occur to them to do so for up to two weeks (Glassman & Anderson, 1999).
In sum, according to its classical definition, transference is merely a repetition of wishes, feelings, fantasies, attitudes, and bodily sensations initially experienced in relation to early-childhood figures and now inappropriately and unconsciously displaced to the therapeutic setting. The client’s transferential experience is something like this: “I want an accepting, non-critical mother, and I do not perceive you as one, therapist. I perceive you as no different from my actual mother. Consequently, I feel the same negative feelings toward you that I felt toward her.”
According to the classical definition of transference, the fantasy that begins and sustains transference can be accounted for by similarities between the therapist and an early-life significant other. The client’s here-and-now experience of the therapist and the client’s there-and-then experience of another become temporarily identical (Nunberg, 1951). The past is reconstructed in the present as the client regresses to an early-life stage, notices similarities between the therapist and the early-life figure, and allows those similarities to guide perception. The therapist is perceived as so similar to a person in the past that he or she is the same person. Thus the therapist becomes a person with whom the client is still conflicted (Freud, 1940).
In other words, the past predetermines the present in that clients cannot help but perceive their revived ideas, feelings, and sensations as simply present realities (Chodorow, 1996). Transference just happens when something in clients’ experience of their therapist, usually of a sensory nature, serves as a reminder of a similar experience recorded in the clients’ memory. Even slight resemblances such as body scents, facial hues and features, gestures, tone of voice, or similarity in names become “kernels of truth” (DeLaCour, 1985) that allow clients to re-experience the entire pattern of their relationship with another person who is still significant on an unconscious level. They even sense the setting and atmosphere in which an encounter with the original person occurred (Rioch, 1943).
For example, “My critical mother had piercing eyes,” the client recalls on an unconscious level, “and so does my therapist. My therapist seems to be my critical mother. She is her.” The stage has been set (Anderson and Przybylinski, 2012). The play can – and does – go on.
Thus “transference is its own motivation;” [it is] “a built-in pattern that impels [clients] to engage in a particular type of similarity-judging, memory-priming pattern of behavior” (Levin, 1997, 1141). It is driven by a compulsion that Freud (1912) termed a repetition compulsion.
Transference as Positive and/or Negative
Originally, Freud (1912) regarded transference as either positive or negative. Either its inherent conflict is overshadowed by pleasant or enjoyable feelings, or it is inundated by disturbing or painful feelings. In the case of positive transference, Freud (1912) believed that clients transfer the needs that a past figure did not meet to their therapist, hoping that the therapist will meet them. A healthy part of the client hopes to create an outcome different from experience. That part wants the present to be better than the past. So more often than not, clients idealize their therapist (Churchill & Ridenour, 2019). In the case of negative transference, in projecting their negative feelings toward a past figure onto their therapist, clients sustain their fear that their therapist will behave like the past figure. An unhealthy part of the client has a desire to repeat what is known, even if it is harmful, because it is familiar and safe (Stark, 1994). The client is invested in keeping things as they were. Indeed, clinical evidence supports the conclusion that “when negative transference predominates, the therapeutic relationship and its effectiveness will be diminished if the therapist does not aid the [client] in gaining an understanding of the sources of the negative experience and perceptions. In the absence of insight, [clients] will simply accept the accuracy and credibility of their negative projections on the therapist …. [They will] … simply believe that the therapist thinks or feels negatively toward [them] or that [their] negative reactions to [their therapist are] warranted” (Gelso & Bhatia, 2012, 388).
Freud (1912) advised therapists to simply ignore positive transference. Or they could regard it as an asset because it had the potential to help form the therapeutic alliance. In contrast, therapists were to interpret negative transference because it was a liability that, left alone, would weaken or destroy the therapeutic alliance.
In time, however, clinicians found that positive transference was very potent. It proved even stronger and more enduring than negative transference (Berk & Anderson, 2000). It also proved to be more subtle and therefore difficult to detect (Anderson & Przybylinski, 2012) and thus detrimental. For instance, it could encourage a culturally re-enforced “gentleman’s agreement” (Wolstein, 1996, 507) to keep the therapeutic relationship non-confrontational and thereby avoid difficult conflict-resolution work.
Hence, even some early Freudian theorists advocated interpreting positive transference if it seemed to interfere with therapeutic work. Equally important, they began to note that negative transference could become a positive experience if therapists were able to make their clients aware of their transference and embark upon the hard work of conflict resolution. 4
Transference as Conflictual
Though a paradigm shift within
psychoanalysis has de-emphasized conflict in transferred material (Anderson
& Przybylinski, 2012; Olds, 1994), the concept of conflict remains central
to the original classical definition of transference. Transferential conflict is
an incompatibility of conflicting desires “such that satisfaction of one such
motive has a negative influence on another” (Westen, 1988, 172). Satisfaction
of a sexual wish, for instance, can conflict with one’s moral values.
Transferential conflict can also arise
from a significant difference between what one needs or wishes and what one
gets. A child who needs protection from a parent, for example, and is instead
neglected, will experience conflict. The child will find it difficult to
reconcile his need to be protected with the neglect he experiences, thinking,
“Should I not need protection?" Or “Shouldn’t I get the protection that I
need?”
Conflict is to be expected even from a
neuroscientific perspective because wishes, beliefs, values, and goals are likely
to be processed by relatively independent neural circuits. In addition, each
hemisphere of the brain forms two independent self-representations or
self-images, one stored in the left and one in the right, that are used again
and again in new situations. Clients can wish for something that their right
brain likes even as their left brain tells them it is illogical to have that
wish. Similarly, clients can choose to endure what they experience as harmful
even though it is painful. For example, to keep some kind of relationship with
a parent, which would be in line with their right brain image of who they are
in a family, clients can allow themselves to continue to endure neglect at the
hands of that parent, which would be a violation of their left brain image of
themselves as rational and therefore not wanting to endure painful neglect.
Clients
who are engaged in transference attempt to dissipate its inherent conflict by
repressing their memory of it or blocking it out of consciousness. They hope to
stop realizing that they have desired a relationship with a neglectful parent,
for example, or have been neglected because they kept a relationship with the
parent. This, of course, lays the groundwork for the phenomenon of transference
to occur when new, similar circumstances remind clients of their old desires or
experiences of not having their needs met. When their therapist has to cancel
their appointment because of an avoidable emergency, for example, clients will
recall the times they were neglected, and thus will feel overwhelmingly
neglected by their therapist.
Transference: Totalistic Definition
The totalistic definition of transference, which is broader than its classical counterpart, was actually formulated early on as Freud’s contemporaries disagreed about whether transference should be restricted to displacement of phenomena from the early past. Jung (1905/1906), for example, saw transference as clients’ unconscious displacement of their relationships with others from any time in their lives.
Others asked if transference could not also be based on clients’ experiences occurring outside the therapeutic setting? Could it not be interpersonal in addition to intrapsychic in that the therapist participated in, contributed to, or even instigated its formation? Indeed, if transference were to be a useful construct during actual therapy, should it not include these experiences and interactions?
Indeed, as early Freudians focused on parental figure links to patterns revealed in the transference, they found it even more important to focus on clients’ reactions to their therapists – as representing others in their present life – than to help clients discover the early-life origins of their problems.
Early Freudians also noticed that emphasizing the early-life sources of transferential patterns could strip clients of defenses they still needed for functioning (Bauer & Mills, 1989). They might not be able to face the fact that the parent who was more protective of them than the other parent failed to do so on a very significant occasion. They might need to defend themselves against that painful realization by engaging in reaction formation, a defense that has allowed them to keep, even embellish, positive aspects of their parent’s image. However, as adults, they had the resources to deal with how someone in the present, namely their therapist, was disappointing them.
Early Freudians also noticed that conflictual material was at least implied in issues that brought clients into therapy. Moreover, tensions and conflicts that occurred during therapy were strikingly similar to those occurring outside of it, making therapy a virtual “slice of life.” It was a slice of a particular client’s life abetted by a particular therapist.
Hence, by the mid-1920s, Rank and Ferenczi (1925) theorized that focusing on displaced material that was impacting the therapist-client relationship – a here-and-now phenomenon – would eventually expose earlier conflicts still needing to be resolved. They seriously questioned whether positive therapeutic outcomes depended solely or even primarily on resolving the early childhood conflicts revealed in transference.
5
Thus for most theorists and therapists, including Freud, the concept of transference eventually acquired a more inclusive meaning that is now its totalistic definition. Transference was the client’s unconscious displacement of attitudes, feelings, sensations, and thoughts from another person in the client’s life – past or present, within the therapeutic setting or outside it – to the therapist in an attempt to re-enact and resolve conflict.
The totalistic definition of transference becomes clearer when contrasted with the classical definition, point by point. Note that the elements they share are not re-examined.
Transference: A Re-Enactment
In the totalistic tradition, transference is a re-enactment rather than a repetition. Motivated by a powerful desire for positive outcome, clients unconsciously assign roles and functions previously taken by others to their therapist in the hope that their needs will finally be met. Clients who unconsciously desire “role-relationship” with another demand “role-responsiveness” of their therapist (Sandler, 1976, 44). They insist that their therapist be an active participant. They prod, provoke, and coerce. As a result of this manipulation, their therapist unconsciously participates. Thus the client “actualize[s] an internal scenario within the therapeutic relationship that results in [the therapist] being drawn into playing a role scripted by [the client’s] internal world” (Westen & Gabbard, 2002, 101) in their unconscious effort to resolve conflict.
Especially tell-tale of this interpersonal dynamic are powerful emotional reactions in therapists that make them step out of their customary roles. So is their clients becoming self-destructive, noticeably foolish, or acting in wild, exaggerated ways (Weiss, 1993).
Clients also set up re-enactments in an unconscious effort to disprove long-held, pathological beliefs, particularly those about their self-identity and self-esteem (Gazzillo et al, 2019). Clients “are highly motivated, both consciously and unconsciously, to disconfirm [their pathogenic beliefs] and get better” (174). Moreover, they have a more or less articulated, albeit unconscious, plan for doing so (Gazzillo et al, 2019; Weiss, 1998). For example, they want their therapist to respond to them in such a way that they can believe they are valuable and competent. Thus they use transference to test reality, saying to themselves “If I am helpless, then my therapist will take over and solve my problems. If not, she will return them to me so that
I take responsibility for doing so.” As Cooper (1987, 518) puts it so well, transference is an “adventure from which [clients hope to] emerge changed and renewed.”
6
The totalistic transference emphasizes the therapist’s unconscious participation through a phenomenon called countertransference. It is an integral part of a transference phenomenon. Transference provokes countertransference (Racker, 1968). Similarly, countertransference provokes transference.
Thus transferential-countertransferential re-enactment underscores an early observation of Freud himself: “It is a fundamental demand of all transference, underlying all the particular demands, that [the therapist] … should participate in a world endowed with particular meaning” (Freud, 1900, 747). As the client unconsciously attempts to re-animate problematic interpersonal relationships, the therapist unconsciously cooperates. Client and therapist become enmeshed in a complex interaction, “a kind of psychic force field compounded out of intermingled transference and countertransference processes” (Meissner, 1996, 42). The transferential-countertransferential “dialogue” between client and therapist serves as a bridge between them, observed Ferenczi (Fleischer, 2023).
Transference: A Dynamic Phenomenon
According to its totalistic definition, transference is dynamic rather than static. It evolves as clients derive positive or negative meaning from their therapists’ seemingly benevolent or malevolent words and actions. Noticing such indicators of attitude as voice quality, degree of energy, level of professionalism, and person-to-person warmth, clients quickly project their feelings and attitudes toward pre- or non-therapeutic persons onto their therapist. Moreover, they see to it that their projections become forceful and intense when they encounter a particular therapist who has traits they associate with their relational conflicts.
Seen in a slightly different light, totalistic transference is dynamic in that it is an organizing activity in which clients unconsciously engage in response to a number of variables: early-life and later-life memories of others, current experiences with others, and the attitudes, words, and actual behaviors of therapists in the present (Stolorow, 1993). Clients impose the organization of prior perception upon the present. They actively, though unconsciously, shape here-and-now psychic reality.
6 They structure and
organize present experience in such a way that the past can come alive and be
re-enacted (Bachant & Adler, 1997). They want the psychic pain they still
hold to disappear.
In other words, totalistic transference is
not simply a matter of clients unconsciously reviving old pictures, thoughts,
emotions, and sensations and perceiving them as present reality. It is not
just, “You seem to be my parent.” Rather, it is “You are my parent. I
know so. I say so. Furthermore, you will love me as a parent and take away my
pain.” Said simply, in the totalistic tradition, transference is an unconscious
insistence that memories of others’ past negative behaviors get replaced by positive
experiences with present-day others. 7
Indeed, totalistic transference is dynamic
in that it is a two-fold process in which therapists unwittingly engage. First,
they act in such a way that they offer clients an opportunity to re-enact past
or non-therapeutic relationships. Their characteristics, interpersonal
behavioral patterns, and traits make transferential role-playing possible. They
actually inspire the very roles their clients project. They collaborate with
clients in writing scripts for the roles they will be asked to play.
Second, as their own transference – referred
to as countertransference – is triggered, therapists with a corresponding
unresolved conflict unconsciously transform the roles their clients assign them
in subtle, idiosyncratic ways. They shape a transference enactment by
responding subjectively to the projections they receive. They give their clients
“additional material” with which they can continue to enact transference.
Therapists who indicate that they even slightly disagree with something their
clients say, for example, permit their clients to embellish their projection of
their critical mother. 8
Recall that the classical definition
already implies that therapists provide “kernels of truth” (DeLaCour, 1985) for
clients. While consciously performing their roles, therapists also
unconsciously contribute other, fragmentary, disguised variables that serve as
reminders of persons in clients’ conflictual past. 9 Therapists momentarily use a harsh voice, for instance, and thus give clients
the cue they needed to notice similarities between therapists and
persons outside therapy who verbally abused them.
However,
the newer totalistic definition goes on to add that clients unconsciously send
a message to therapists that they have already activated their potential to
take the role now being assigned them. 10 Those who could be critical, for example, are already being perceived as critical.
Therapists then unconsciously introject the message and, if their
countertransference permits it, enact the role of a critical person. They might
use a slightly disparaging tone of voice, for instance, or use it to a greater
degree than usual. 11 Thus the totalistic definition of transference emphasizes the powerful
influence that therapists’ personal, countertransference-based characteristics
and behavior have on the content and shape of clients’ transference (Cooper,
1987).
Transference: A Displacement of
Interpersonal Experience
Totalistic transference is displacement of
any interpersonal experience in life, not just early-life experience. It adds
the recent past to the early past as well as the present to the past as sources
of clients’ conflicts (Strachey, 1934, 1969). The totalistic definition of
transference adds what is going on interpersonally outside of sessions to what
is transpiring in sessions and adds what has been going on
intrapsychically in the client since infancy. An example would be the
increasingly common negative perception of immigrants in the U.S. As
Tummala-Narra (2019) points out, “Perceptions of [immigrants] … based on
projections of unwanted parts of the self … are becoming justifications for the
demonization of racial minorities.” (4) 12
With Jungian theorists, the totalistic
definition of transference has become so broad that it includes archetypal
phenomena: universal and transpersonal material common to humanity throughout
the ages and therefore able to serve as prototypic interpersonal templates.
Universal archetypes trigger transference, and transpersonal archetypal themes
form its content. Age-old, worldwide, collective, and transcultural material
emerges as the client’s own (Jung, 1966). The archetypes reveal their powerful
relevance in generation after generation, culture after culture, and individual
after individual (Dieckmann, 1976).
Thus, according to Jungians, transference
is both a new experience and an enactment of an old one, be it unique to the
individual or inherited. It is a here-and-now personal phenomenon based on a
then-and-there universal memory. “I am an older sibling in competition with my
therapist, my younger sibling,” a client fantasizes, for instance, in response
to a trigger related to scarcity and universalized in the Sibling Rivalry
Archetype.
A Description of Transference for Non-Analysts
The following description of transference
will serve as its definition in the rest of this course. It is an
operationalized definition that provides a concrete template by means of which
non-analysts can verify suspected transference phenomena.
Transference is matter of the following:
- Clients
unconsciously and compulsively attempt to re-enact in therapy unresolved
interpersonal conflicts originating in the past or outside of therapy, along
with conflicts they hold because of archetypal phenomena.
- Clients
unconsciously attend to similarities between their therapists and others with
whom they have unresolved conflicts during their therapy sessions. They then
let these similarities motivate them to displace past phenomena to the present
therapeutic setting. They project qualities of other persons onto their
therapists.
- Clients
unconsciously organize their relationship with their therapist during sessions
in such a way that, without consciously addressing past or present conflicts,
they can reduce or eliminate their emotional pain.
- Clients
assign to their therapists roles originally played by significant others with
whom clients are still conflicted. They attempt to re-enact conflictual
experiences and have them “turn out well.”
- Concurrently, therapists introject or unconsciously take in their clients’ projections:
messages that they are like others and behave as they did.
- Concurrently, clients unconsciously permit their therapist to project to them pre- and
extra-therapeutic material that they can develop into transference phenomena.
- Both clients and therapists unconsciously permit themselves to be influenced by
universal archetypes that suggest they play certain roles and assign
corresponding roles to each other.
The Phenomenon Called Countertransference
Countertransference: Classical Definition
Classical countertransference is a mirror of classical transference. It is therapists’ own transference being elicited by clients’ transference (Freud, 1910). It is therapists’ feelings and attitudes toward a significant early-life figure being displaced to the client (Freud, 1912).
When defined as a construct, countertransference refers to therapists’ unconscious reactions to clients’ feelings and attitudes toward a significant past figure being displaced by therapists themselves. It is an automatic reaction quickly triggered by therapists’ own unresolved conflicts.
In other words, countertransference is a matter of therapists’ repressed, early-life, unresolved conflictual feelings and attitudes that surface as they experience clients’ displaced conflicts. Countertransference is a fusion of past and present. When old material is transferred to the therapeutic setting, the past becomes the present.
When defined as a process, classical countertransference refers to clients’ transferential communication “calling forth” from their therapists’ unconscious mind feelings and attitudes related to their own early-life conflictual experiences. Although there can be some exceptions, ordinarily this “calling forth” depends on two dynamics.
One is that clients unconsciously send memories of early-life conflictual experiences to their therapist’s unconscious mind, and the therapist unconsciously receives them. Neuroscientist Olnick (1969) explains that therapists’ right-brain communication receptors are tuned in to their clients’ right-brain communication expressions. Using subliminal sensory signals, clients project onto their receptive therapists the traits or habits of persons that led to the clients’ early-life conflicts.
The second dynamic on which “calling forth” depends is that therapists already have unconscious memories of their own early-life conflictual experiences that can be “called forth” by clients’ transference. They have conflict-based templates that permit them to transfer presuppositions or presumptions to the therapeutic setting (Herron & Rouslin, 1982). “You are a sibling who has bullied me and are about to do so now,” a therapist unconsciously thinks about a client who has projected onto him the traits of a sibling who once victimized him. Thus countertransference “is determined by the fit between what [the client] projects onto the therapist and what preexisting structures are present in the therapist’s intrapsychic world” (Gabbard, 2001, 9).
In the classical tradition, countertransference refers
only to those reactions caused by displaced psychic conflicts that clients have transferred from an early-life relationship to the therapeutic relationship and that therapists still have with persons from
their early years. These conflicts are triggered by right-hemispheric, non-verbal communications of clients and therapists, but they are not based
primarily on what occurred during therapy sessions. Consequently, they are not justifiable in terms of objective data. They are inappropriate or irrational. Therapists may be annoyed by clients who come late for a session, for example. But if countertransference is not at work, therapists are not outraged. On the other hand, if therapists were frequently kept waiting because of the insensitivity of a parent and they are transferring that attribute to their clients, they become outraged.
13
Countertransference,
like transference, is subject to a habit of the unconscious mind called repetition
compulsion. Because of repeated projection and introjection, feelings and
attitudes in the therapist’s unconscious mind are easily and quickly re-activated.
They are not subjected to reality testing but simply make therapists
unconsciously re-use old perceptions and re-make old judgments. They set the stage on which therapy plays out.
It is generally presumed that therapists
introject or unwittingly take in clients’ projections before clients introject
therapists’ projections. However, it is more likely that introjection, like
projection, is a simultaneous activity of therapists and clients. Or, clients
may introject first as therapists provide “kernels of truth” on which clients
can base their transference. These “kernels” may
be not only the therapist’s piercing eyes – which are like the client’s mother’s
eyes – but also the therapist’s subtle habit of criticizing others that
corresponds to her client’s schema of mothers as persons who invariably find
something wrong with their child. Indeed, in the classical definition,
countertransference is a matter of clients’ transference activating therapists’
unconscious templates of what life and people are like because of therapists’
own early-life unmet needs and unfulfilled wishes.
Countertransference occurs automatically.
Then, as soon as it is suspected by the conscious mind, it is itself repressed
or dismissed. Signs of its presence, called derivatives or manifestations, may be noted by the conscious mind – the therapist may become aware of shuddering
in disgust, for example – but countertransference as such takes place within the
inaccessible realm of the unconscious mind. That part of the psyche, which is
simply called the unconscious, is a “receptive organ” (Freud, 1912, 115) or
“delicate receiving apparatus” (Money-Kryle, 1956, 341) that has no choice but
to introject what another person projects. It is unable to use the conscious mind’s
reality-testing function to distinguish between fantasies of its own making and
objective reality. It fuses past and present. It incorporates one person within
another. It distorts perception, impairs insight, and clouds judgment.
Hence a therapy scenario such as this. The conscious mind knows “I am not this client’s younger sibling,” even as the more influential unconscious mind concludes, “Because I feel like my client’s younger sibling, I am him.”
In sum, classical countertransference occurs because of therapists’ conflictual wishes and needs. Therapists who have not resolved their conflict between their wish for their mother’s unconditional love and her real-life withholding of love, for example, tend to experience older, maternal clients as limited in their //ability to cherish others, including their therapist. This, in turn, informs the therapists’ attitude and behavior toward these clients. They feel distanced from their clients. They withdraw from them. They minimize their verbal interactions with them. Thus unless countertransference is detected and processed by the therapist's conscious mind, it is very likely to undermine positive therapeutic outcome. If detected and worked with, however, countertransference can lead to a positive therapeutic outcome. Like transference, it is a double-edged sword.
Countertransference: Totalistic Definition
Countertransference becomes even more
complex in its totalistic definition. Because of widespread disagreement on how
totalistic countertransference is defined, we will explore just two
representative definitions.
At the start, it is important to note that
these two definitions, like most totalistic definitions,
presume the following three elements of the classical definition. First,
therapists’ countertransference takes the form of emotions, sensations, and
cognitions related to their clients. Second, countertransference involves
unresolved conflict that has been repressed in the unconscious mind of therapists.
Third, besides being dependent on projection and introjection,
countertransference is also dependent on identification, a phenomenon
wherein clients and therapist actually see parts or aspects of the other person
as belonging to themselves. They identify it as their own.
The Broadest Definition
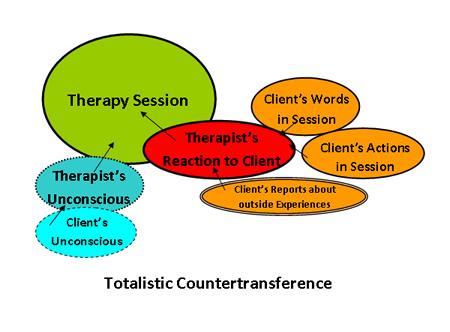
According to Heimann (1950), totalistic
countertransference refers to all attitudes and feelings that therapists
experience toward clients, unconscious as well as conscious. It is the total
reaction of therapists to their clients in the therapeutic setting. It
consists of therapists’ unconscious, unresolved conflicts that are elicited by
clients’ transference, as well as therapists’ conscious, justifiable reactions
to actual experiences during therapy. It includes reactions to what clients say
and do in therapy and to what they report they are going through outside of
therapy (Kernberg, 1987).
Thus the broadest definition does not limit countertransference to unconscious, early-life material, to the past, to the subjective, or to fantasy. Rather, it is therapists’ response both to real attributes of clients and to attributes that therapists merely fantasize. A client might indeed be boorish, but a therapist might label him as boorish simply because he resembles a boorish person in the therapist’s past. Likewise, especially with Jung (1905/1906), countertransference is a reaction to present and recent material no less than early-life material. For example, if therapists are being glorified by interns whom they supervise, they might unconsciously assign similar adulatory roles to their clients. Then, when clients do not admire them, they are disappointed.
In other words, totalistic countertransference, which is subjective in that it arises within the mind of the therapist, may also have an objective component in so far as it is a reaction to clients’ actual behavior in sessions. It is a product of the present therapeutic relationship as well as the past and present non-therapeutic relationships that both clients and therapists transfer to their therapeutic encounter.
Interesting new research supports the theory that totalistic countertransference is neither rare nor infrequent. Gazzillo and colleagues (2015), for example, have found that the emotional reaction of all 144 clinicians studied to clients with personality disorders was helplessness, with the degree of helplessness dependent on the level of the client’s overall pathology. Furthermore, clinicians’ reaction to clients with a histrionic personality disorder was a feeling of being overwhelmed and sexualized. Their reaction to clients with narcissistic personality disorders was a desire to be parental even as they felt humiliated. Their reaction to clients with phobic personality disorders was simply a desire to be parental.
In its broadest sense, totalistic
countertransference consists of affect, cognition, and bodily sensations
stemming from unmet needs of both therapists and clients. It is
occasioned by what clients do to therapists both knowingly and
unknowingly. It is sparked both by what therapists bring to sessions
independently – what is “set to go” – because of therapists’ previously fashioned
conscious and unconscious schemas regarding people and by the professional
roles that therapists believe they must play. They may transfer a maternal role
to the therapeutic session, for example, when working with a distraught client
who strikes them as child-like.
Totalistic countertransference is a matter
of therapists’ experiencing toward clients the feelings and attitudes that
therapists originally associated with other persons with whom they still have
problematic interactions (Racker, 1968). It is also a matter of therapists’
unconsciously assigning to clients roles peculiar to their own interpersonal
experiences and the ways they define themselves in the present. Therapists send
messages “asking” their clients to take certain roles that will meet their
still-unmet needs and fulfill their still-unfulfilled wishes.
For example, therapists who have suffered
from dominating fathers tend to assign a dominating role to their clients,
usually older males, in the hope that their clients will choose not to
dominate. Thus they will meet the therapists’ long-held need for
self-determination. Similarly, therapists who see their role as quasi-medical
tend to assign patient roles to their clients. They give them a chance to be
healed and thereby fulfill their desire to heal others.
Of course, therapists’ countertransference
also creates opportunities for clients’ transference. In behaving in certain
ways on their own, therapists create opportunities for clients to relate to
them in ways reminiscent of clients’ relationships: early, later, and
contemporary. As recipients of therapists’ behavioral tactics, clients
experience their own unresolved conflicts and re-discover aspects of their
conflicted selves. Therapists who are somewhat authoritarian, for example,
enable clients to return to a student role if that role has remained
conflictual for them. In the countertransference, clients find themselves,
Sandler (1976) says succinctly.
In addition, in its broadest sense,
totalistic countertransference includes transpersonal and transcultural
archetypes that emerge as therapists’ own material and get transferred to the
therapeutic setting. In fact, according to Jung (1966), archetypes are the
major triggers of both transference and countertransference. Therapists might
regard themselves as superior to their clients, for example, because of the God
and Goddess Archetype. They might classify clients as inferior to them even as
therapy begins or do so at the time clients transfer their tendency to become a
victim from an early-life situation to the therapeutic setting.
Racker (1968) believed that totalistic
countertransference depends not only on projection and introjection but on identification: a phenomenon whereby clients and therapists actually see parts or aspects
of the other person as belonging to themselves. Identification includes (1)
projective identification, a mental activity engaged in by one person; and (2)
introjective identification, a corresponding mental activity engaged in by
another person. In analytic tradition, projective identification is attributed
to the client and introjective identification, to the therapist.
Klein (1946) first defined projective identification as children’s fantasies of ridding themselves of unwanted feelings by assigning them to someone else. Today, however, most theorists define projective identification as the omnipotent fantasy that we can split off an undesirable part of our personality, put it and emotions that it incites into another person, and then recover a modified version of what was put into the other person (Grinberg, 1962; Ogden, 1982). Because we unconsciously pressure others to identify with or own what they receive, and that they ordinarily succumb to that pressure, we experience a feeling of oneness with those persons (Schafer, 1977).
Schore (2003a) adds that those engaging in projective identification become dependent on the persons into whom they project the unwanted part. They need the persons to learn how to deal with the part. They might even need to collaborate with the recipients to manage it. For instance, clients who have anger management problems first unconsciously put their anger into their therapist. They then unconsciously observe what their therapist does with the anger. They note how the therapist momentarily stops talking, for example, so that she will be calm when she says something. Interestingly, clients will unconsciously talk in a very calm way to help their therapist regain composure.
In the course of projective identification, clients unconsciously put into their therapist a part of their identity that they are unable or unwilling to own as theirs. Concurrently, the therapist participates by unconsciously internalizing that part in a process called introjective identification.
Clients use projective identification to put into their therapist a distressful part of themselves for one of two reasons (Hinshelwood, 1999). The first is that the distressful part is related to memories of an experience in which others treated them badly, which implied that they were bad persons. The second is that the distressful part is the cause of the clients' treating someone else badly, which also implies that they are bad persons and makes them not want to own what they are doing and the guilt it carries. It is either, “You are abusing me and therefore distressing me. I must be a bad person;” or “I am treating you badly and cannot stand that in myself. I cannot stand being a bad person.”
When they become recipients of what their clients’ project, therapists identify with their clients and/or with those who have been affected by them. Grayer and Sax (1986) note that in any given session, therapists usually move back and forth; identifying first with the client, then with a person affected by the client, then with the client, and so forth.
Projective identification is a three-step process that occurs quickly. First, clients unconsciously put into their therapist an undesirable part of themselves to defend themselves against psychic pain (Ogden, 1982). They unconsciously scapegoat: place into their therapist something in them that feels so unbearable that it must be expelled (Heath, 1991). Indeed, they do this so completely and so unwittingly that they attribute what they expel no longer to themselves but to their therapist. Abusive clients who are unable to tolerate that trait in themselves, for example, engage in projective identification by perceiving their therapist as abusive. In that way, they experience their therapist, not themselves, as abusive.
Second, clients exert pressure on their therapists to experience themselves and behave in a way congruent with the projective fantasy they have received (Ogden, 1994). Clients stimulate in their therapists intense, unexplained, and ego-dystonic emotions (Maroda, 1995) which cause them to undergo an affective experience in line with what they receive. They feel abusive, for example, and detest it (Kernberg, 1987). Moreover, as therapists resonate with what they have received, they internally amplify the emotions connected with it (Schore, 2003a). They become very distressed without understanding why. They find it difficult to put into words what is going on.
For that reason, projective identification is considered a form of non-verbal communication. By placing the pain of being abused into their therapist, for example, clients enable their therapist to know by experience how painful it was for them to be abused. This is particularly important to clients when they cannot describe an experience. Consider the following vignette:
In his therapy session, the client denied being sexually abused. In fact, he laughed when he heard the suggestion that others with his symptoms usually have been sexualized at an inappropriate age. Yet his therapist experienced a vague, partly comfortable, partly uncomfortable sexual attraction to her client. It was not as if she perceived the client as physically attractive; it was simply an attraction “out there” by itself.
In time, when the therapist disclosed her countertransferential reaction, the client revealed that he had engaged in sexual play at age five with a babysitter. He enjoyed it, he said, even though he had no other fond memories of the person.
As the therapist and her client talked about what had occurred when he was a child, it became clear to her that what happened to her in therapy was an enactment. She realized that though her client said he enjoyed it, in fact he was conflicted over it. He enjoyed what he later learned he was not supposed to do. When he placed into his therapist his projective fantasy of having a sexual relationship with her, however, he could enjoy the memory of the original experience without having to own it.
Third, clients who are engaged in projective identification unconsciously attempt to recover the part they have expelled. They want to get the feel of what their therapist has gone through. They want to know what the expelled part is like now that the therapist has had to deal with it. They sense that their therapist has actually felt what they themselves could not tolerate and has not only tolerated it but also dealt effectively with it. As a consequence, the part is less terrifying, and their negative feelings are either gone or at least more manageable (Ogden, 1994). In the above vignette, for instance, the client would have sensed that that his therapist managed the sexual fantasy he had projected.
Thus by using projective identification, clients are able to fantasize
that they can safely take back or re-own their original experience. They will be able to benefit from their therapist’s modeling. They will be able to manage feeling controlled, for example, by rebelling against it, as did their therapist. Although negatively affected by a client’s projection, the therapist has managed to contain it (Pick, 1985).
14 Now, in a safe interpersonal environment, the client can “metabolize” a
negative emotion into something positive (Schore, 2003b).
It is not always the case, however, that therapists adaptively manage the feelings they have introjected. If they cannot tolerate them, they confirm clients’ belief that their feelings are indeed unbearable and unmanageable. Then clients feel even worse. They experience hopelessness and despair (Bion, 1967).
According to Grinberg (1962), who was among the first to link projective identification with countertransference, projective identification accounts for transference-countertransference enactment and role-responsiveness. Projective identification is a form of pressure exerted by clients to get their therapist to help them process affective experiences that they have not been able to deal with (Schore, 2003a). In that the therapist becomes as much an active participant as the client (Plakun, 1998), projective identification is interpersonal, rather than merely intrapsychic, as Melanie Klein (1946) conceived it.
A close look at introjective identification, an unconscious process whereby therapists experience a feeling state that clients have put into them in an attempt to disown it, reveals significant challenges for therapists. It takes one of two forms as therapists identify with what they have received and own it as their own.
In the first, called concordant identification, therapists feel like their client. They feel abused, for example, and sorry for the client who has been abused by her mother. The client’s subjective reality seems to the therapists to be based in their own current reality. Thus concordant introjective identification increases therapists’ empathy for their clients.
In the second, called complementary identification, however, therapists feel the impact of what the client has done to another person. They experience what the recipient of the client’s actions has experienced. As a consequence, they empathize not with the client but with the person with whom the client has interacted. To use the last example, the therapist experiences the frustration of the mother who resorts to abusing an obstinate child.
With this, there is good news and bad news. The good news is that the experience yields valuable information regarding what clients have contributed to their problems. The bad news is that therapists must now struggle with mysterious, unexplainable negative feelings toward their client. Unless they quickly process those feelings, they will enact them, giving their client additional psychic pain.
Even if concordant identification is therapists’ reaction, they cannot do psychological work for their clients. Being empathized with can mediate healing, but that healing will be temporary unless clients learn to heal themselves, which they can do if they face their pain, process it, and, in most cases, change what they do to prevent its reoccurrence. That might be refusing to accept victimhood as a fundamental self-identifying label for example, in the case of having actually been victimized and being victimized in the present.
In other words, only when clients become aware of the conflict inherent in transference and embark upon the hard work of conflict resolution can they free themselves from the pain of abuse.
15 That pain remains because the past becomes the present through a repetition
compulsion at the core of transference (Freud, 1912).
A Narrower Definition
Some theorists, such as Blum (1986a), find
countertransference’s totalistic definition so all-encompassing that it is
difficult to use in clinical settings. Consequently, they offer one that is
less comprehensive: countertransference is only those feelings and attitudes that
are unconscious, irrational, and inappropriate because they are displaced;
and it is only those that are conflictual or problematic.
If clients actually act badly in the
session and therapists get angry, that reaction is called a counter-reaction,
not countertransference. If, on the other hand, clients project onto therapists
an early-life “picture” of themselves as acting badly but do not actually act
badly in the session, and therapists introject that old “picture,” their angry
reaction is termed countertransference. Thus countertransference is
labeled irrational and inappropriate; it defies logic, strictly speaking. The present is not the past.16 One person is not another, however
much they resemble each other.
In other words, countertransference is a matter of the imagined or fantasized perceptions of which therapists are unaware. It is composed only of unconscious reactions.
Furthermore, countertransference involves only conflict-based reactions of therapists. If a therapist has resolved her
conflict over expecting her mother to meet her needs and finding her mother
instead neglectful, projection – but not countertransference – will occur. The
client who resembles a mother might project her own unresolved conflict related
to neglect, but the therapist will not feel neglected, at least not appreciably.
Descriptors of Countertransference
Whether defined classically or totalistically,
countertransference can be described in the following ways.
Countertransference Is Subtle
Though signs or manifestations of
countertransference are occasionally easily detectible, they are usually very
subtle. They tend to be disguised or vague feelings, desires, images, gestures,
fantasies, associations, bodily sensations, and urges to respond differently
from the way one usually does. They might take the form of silence, boredom,
fatigue, fragmentary thoughts, and various combinations of these phenomena
(Grayer & Sax, 1986). In response to a client who dislikes women, for
example, a female therapist might feel chest pains or have difficulty speaking.
Or she may see an image of a person she dislikes. She may feel humiliated. She
may desire to end the session.
Even therapists who make every effort to
be nice can give subtle clues regarding their co-occurring negative feelings.
As clients pick them up, even strong positive transference can turn negative
(Anderson & Przybylinski, 2012).
Countertransference Is Unique and Varied
Like transference, countertransference
takes many unique forms in every client-therapist relationship. It would be
more accurate to say there are countertransferences rather than
countertransference. Particular clients remind therapists of other persons, and
therapists unconsciously impose idiosyncratic templates on the therapeutic
relationship and assign specific roles to their clients. In addition, when
clients and therapists represent different ages, ethnic groups, genders,
religions, political affiliations, and socio-economic strata, their effect upon
each other is highly distinctive. Even with the same therapist-client dyad, in
no two sessions do countertransference phenomena tend to be identical. This is
especially true of clients with personality disorders (Hennissen, 2019).
Countertransference Is Both Simple and Complex
Countertransference, like transference,
involves simplified perceptual and cognitive processes. In order to associate a
client with a person whom a therapist dislikes, for example, the therapist must
dismiss all aspects of both persons except the common trait or behavior the
therapist dislikes. Even before that, the therapist must accept the client’s
transferential message that the therapist reminds him of a disliked person with
whom the therapist has relatively little in common. Perhaps it is his age.
Perhaps it is his age and slightly authoritarian tone of voice. Perhaps it is
his age, authoritarian tone of voice, and similarity in clothes. But it is not
the scores of similarities that justify identifying one person as another.
At the same time, countertransference involves
complex fantasizing. After focusing on select data, therapists go on to embellish
their fantasies. To use the previous example, they might unconsciously add to their
emotion of dislike such “evidence” as physical sensations of being punched in
the chest or an urge to get rid of the client they dislike. Gazzillo and
colleagues’ (2019) research reveals that distress can indeed make people lose
clear thinking and become pseudo-logical or illogical.
Of course, the more therapists acknowledge
and deal with conflictual material in their unconscious, the less they will fantasize
about it. However, it is extremely difficult to complete that work. Thus new
clients can uncannily call forth therapists’ deeply repressed, only partially
examined conflictual material. In fact, though therapists vary in their
susceptibility to countertransferential fantasizing, none manage to avoid it completely
(Herron & Rouslin, 1982).
Countertransference is complex in yet
another way. It is a convoluted process that not only begins with
anxiety-ridden, repressed material, but is itself repressed because of the
additional anxiety it incites. It then re-occurs when similar conditions arise,
only to be pushed into the unconscious once more. Repetition compulsion at
work? Yes.
Countertransference Is Both Positive and Negative
Freud (1910a) originally regarded countertransference as negative. It was therapists’ undesirable reaction to their clients’ transference. Because it interfered with therapeutic work, it was to be roundly dismissed. In time, however, theorists noticed that countertransference was either positive in that it was basically conflict-free or negative in that it was conflict-based.
However, while developing their totalistic definition, theorists realized that countertransference has both negative and positive aspects. On one hand, it ordinarily distresses therapists. They must use energy to repress it. This, in turn, limits insight, clouds thinking, interferes with communication, and leads to misunderstandings that mar treatment.
On the other hand, if detected and decoded, countertransference alerts therapists to what is going on in their relationship with clients (Racker, 1968). It increases therapists’ knowledge of their clients’ personal traits and interpersonal patterns. In fact, some of these traits and patterns are accessible only through therapists’ countertransference reactions (McDougall, 1978; Cohen, 1952).
For this reason, countertransference is an indispensable tool (Ferenczi, 1909). Indeed, it should be the heart of the psychoanalytic method. Along with transference, therapists should let it unfold in their relationship with their clients with all the force of the emotions it activates, for it will find its own resolution as therapist and client openly welcome it and use it for transforming clients’ maladaptive mind-set into one that is adaptive (Jung, 1944).
In sum, countertransference is a double-edged sword with the potential to bring about both negative and positive therapeutic outcomes.
Countertransference Is Governed by Laws of the
Unconscious Mind
Countertransference is governed by an
unconscious law of the human psyche to repress what is anxiety-ridden and thus painful.
It is also governed by what is called the “law of Talion”: react to positive
transference by positive countertransference and to negative transference by
negative countertransference (Racker, 1972). This happens quickly and
automatically, that is, within milliseconds and at levels beneath awareness
(Sternberg et al, 1998). It is not a matter of conscious intent.
Consider, for instance, falling asleep in
a session, which usually makes therapists feel guilty. At least initially,
however, they will attribute their dozing off to clients’ being boring;
bringing up nonessential material or repeating ad nauseam. Because they
are unaware of transferring material themselves, they do not realize that they are retaliating in returning negative countertransference for negative
transference. But this is very likely what is happening in addition to the
client’s actually being boring. When accurately decoded, the
countertransference often yields its Talionic motivation.
Another
law of the unconscious mind to which countertransference is subject is the “law
of elaboration”: build on, flush out, and give detail to your fantasies. Hence,
just as dreams are usually elaborate, confusing, and bewildering,
countertransference prompts therapists to feel and behave in accordance with
the identifications they are making. In subtle and varied ways, they play
elaborate roles and perform detailed functions characteristic of figures in the
past (Bion, 1961). Unconsciously they take their roles to heart and play them
“to the hilt.” That’s the bad news.
Countertransference Can Be Revelational
The good news is that once
countertransference is detected and accurately decoded, it reveals to
therapists how they are influencing the therapeutic process, for better or
worse. If they like the elderly because of their sweet grandparents, for
example, and convey that message to elderly clients, the latter feel valued and
accepted. The therapeutic alliance is smoothly and soundly launched. If, on the
other hand, therapists dislike the elderly because of their disgruntled
grandparents, they tend to perceive their clients in a negative light. Consequently, the latter feel devalued and rejected, and the therapeutic
alliance is fragile at best. Similarly, if therapists continue to associate
their elderly clients with their sweet but failing grandparents, they tend to infantilize
them.
If detected and accurately decoded, however, countertransference gives therapists data about what is going on between them and their clients, as well as about how they and their clients are influencing the therapeutic process. Countertransference opens the door to “slices of life”: the client’s life, the therapist’s life, and the life that client and therapist share in the therapeutic setting. It gives therapists a first-hand experience of what their clients communicate despite their efforts not to.
Indeed, the true message of clients is
understood primarily in what their communication does to therapists. Far more
important than what clients consciously say in therapy are the attitude and
affect with which they unwittingly say it, for in these elements lay both the
fullness of meaning and the impact of clients’ communication on others. “The
way the therapist feels impelled to feel and behave because of the client’s
transference may be as important” as what the client says, and perhaps more
important (Pally, 2001, 91). A client’s “What should I do?” for instance, can
inspire a therapist to give advice, help the client think through alternatives,
or turn the question back to the client, all depending on whether the
therapist’s countertransferential reaction is one of pity for one without
experience being forced to act immediately, confidence in one who desires to
become more analytical, or impatience with one who wants to stay dependent. In
sum, therapists stand to gain their most significant insight into how they need
to plan their work with clients by decoding their own countertransference.
For this reason, countertransference, even
more than transference, has been called the central instrument of therapeutic
work (Brodbeck, 1995). Countertransference is “the map guiding the clinician
through the hidden shoals of the transference” (Davies & Frawley, 1994,
152). Countertransference is the most valuable instrument of research into the
client’s unconscious that the therapist has (Heimann, 1950).
A Definition of Countertransference for Non-Psychoanalysts
The following description of countertransference
will serve as its definition in the rest of this course. It is an
operationalized definition that provides a concrete template by means of which
non-analysts can verify countertransference phenomena they suspect.
Countertransference is matter of the following:
- Countertransference
is an unconscious process whereby therapists “allow” clients’ transferential,
nonverbal communications to elicit their own transference: their unresolved
conflicts. Therapists respond to clients’ transferential communications according
to the significant, conflictual relationships that they, therapists, have
previously or are presently experiencing, or experience because of
archetypal phenomena.
- Countertransference
is an unconscious process whereby therapists attend to similarities between
their clients and others with whom they have unresolved conflicts. This permits
them to displace past or extra-therapeutic conflictual experiences.
- Countertransference
occurs when therapists unconsciously take in clients’ projections and identify
with the clients or with those affected by clients’ verbal and non-verbal
behaviors. They experience the affect once felt by their clients or the
recipients of clients’ behaviors. In the first case, therapists tend to
empathize with clients in the course of experiencing their subjective world. In
the second case, therapists tend to empathize with those with whom clients
relate in the course of experiencing what clients do to them. Thus
countertransference sheds light on how therapists can plan to help clients.
- Countertransference
is an unconscious process whereby therapists assimilate clients into the
thematic structures of their own subjective, conflictual world. Therapists come
to their work with unconscious schema, templates, or images independent of
clients. They unconsciously impose them on clients.
- Countertransference
sheds light on what therapists must do to meet their own needs and fulfill
their own wishes outside of therapy and thereby free themselves for concentration
on clients during therapy. If they fail to do so, therapists will
unconsciously assign to clients roles originally played by significant others
with whom therapists are still conflicted, in an unconscious effort to meet
their own needs and fulfill their own wishes. Their work will be unsuccessful.
They may even behave unethically.
Triggers of Transference and Countertransference
Countless and
varied stimuli trigger transference and countertransference in everyday living.
The realms of the unconscious mind wherein transference and countertransference
“reside” are multi-structured, multi-layered, and multi-faceted. Unconscious
psychological life is no less complex than biological life.
However, during the course of psychotherapy, Jung discovered, transference and countertransference are triggered primarily by what are called archetypes. One explanation is that therapy is a highly interpersonal process that draws from its participants primordial, transcultural interactional patterns, such as taking care of infants and children or appealing to powerful others when in danger. Specific cultures have developed somewhat unique forms of maternal caregiving and turning to those in authority, but all cultures have learned to survive by enacting such archetypes as the Mother Archetypes and the God and Goddess Archetypes.
A second explanation for archetypes
triggering transference and countertransference is that therapists and clients
hold archetypal beliefs about situations that tend to occur in therapy. “Those
in danger of decompensating, for example, must depend on those who know how to
protect and defend them,” clients and therapists unconsciously believe. Hence
the triggering power of the Father Archetype.
Our focus will be on five of the
archetypes that evoke three major dynamics that directly affect the treatment
relationship: attachment and intimacy, authority, and sexuality (Westen &
Gabbard, 2002). Because they appear and reappear in various culture-influenced
forms and intensities during the course of therapy (Dieckman, 1976; Kernberg, 1975),
they can cause “significant distress or impairment in social, occupational, or
other important areas of functioning” (Kupfer, et al., 2013, 21), including
clients’ and therapists’ functioning in the therapeutic setting.
Archetypal Material Is Embedded in Culture
Jung (1966) held that universal themes, collective beliefs, transcultural images, and primitive interpersonal scripts known as archetypes persistently attract the attention of the unconscious mind wherein they reside. Archetypes are actually “symbols of our psyche and understanding ourselves,” (Scott, 2023, 1) Consequently, “they have remarkable influence over our relationships, expectations, and social interactions,” (Scott, 2023, 1).
Indeed, they have become structural elements of the human psyche. They “demand” to be used as patterns for interpersonal interactions. They prompt therapists and clients to resonate with them, even enact them, in the therapeutic setting. Indeed, Schafer (1959) points out, “therapists [and clients] become in certain respects mother, father, sibling, child, and lover [to each other],” (354).
However, the exact nature of transference activity depends on the client’s and therapist’s cultures, with culture being defined broadly to include ethnicity, age, socio-economic class, political affiliation, gender, sexual identity, religion, and other demographic characteristics. For instance, sibling rivalry in a Korean culture defined by a gender and age hierarchy as well as by the influence of in-laws is different from its expression in a single-parent, Anglo-American family culture that emphasizes individual responsibility. Thus therapists must observe archetypal-based transference through lenses of the interwoven and ever-evolving cultures with which a particular client and they themselves identify.
Put succinctly, ethno-cultural transference is a core variable in therapeutic work. Sociocultural histories of both client and therapist influence therapeutic dynamics (Comas-Diaz and Jacobsen, 1991). Individual narratives and interpersonal therapeutic dynamics are without doubt shaped by culture. Consequently, therapists must understand clients’ narratives in terms of “what lies beneath [their] meanings, how and in which context they were formed … and the anxiety [they create in] the client and the therapist” (Tummula-Narra, 2015, 283).
In addition to this, therapists must note long-lasting similarities among cultural identifications. They must also be wary of clients’ manipulation of culture as a defense mechanism. “All Latinos are late,” said by a client who arrives late, for example, may not be a valid excuse as much as an attempt to limit interaction with the therapist because the God and Goddess Archetypes have incited fear in the late-comer.
In addition, therapists must be wary of their own unconscious bias against cultures other than their own. Should they see them as inferior, for example, they may not hold high expectations of clients. They may pathologize them or regard them as too entrenched in their ways to change.
See footnotes following this text for other culture-specific issues.
The Mother Archetype
The Mother Archetype is the most powerful
trigger of transference and countertransference in therapy because it is
tantamount to our need for secure attachment and simple intimacy. It is a
matter of our wanting to be loved unconditionally. It corresponds to our need
to be truly valued, if only by one person. It permits us to discover our
capacity “to light up the mother’s face,” an experience that becomes the
“fundamental basis of self-image and self-esteem” (Casement, 1991, 93). Indeed,
“the human face is … an awesome primary miracle; it naturally paralyzes [one]
by its splendor if you give in to it as the fantastic thing it is” (Becker,
1973, 147).
Concurrently, the Mother Archetype
promotes complementary maternal, care-giving attitudes and behaviors. On the
positive side, these variables are key to establishing the nurturing,
interdependent environment necessary for forming the therapeutic alliance.
Thus as therapy begins, it is not uncommon for clients to regress, becoming psychological children, even infants. For all of their lives – not just as children – they need an attachment figure to provide them safety, comfort, and protection (Bowlby,1982; Kline, et al., 2023). Consequently, they unwittingly give cues that they hold non-verbal expectations of symbolic bodily contact, of being held, fed, and kept warm and dry (Fortuna, 2023, 80-91). Clients, like infants, entertain fantasies of returning to the mother-infant symbiotic state wherein they are no longer separate individuals (Benedek, 1953). They fantasize about a psychological, pseudo-biological merger in which they enjoy undivided attention and unconditional positive regard.
Thus initial transference triggered by the Mother Archetype is usually positive. This is true, perhaps especially true, even for clients who had an abusive mother (Anderson & Przybylinski, 2012).
17 For contrary to all evidence, they still hope to be loved. They “automatically
re-experience” a “positive evaluation” when first interacting with their
therapist (p. 375).
Interestingly, this is the case despite clients picking up equal numbers of negative and positive features of their
therapist as soon as they come in contact. It is just that the positive
transference proves stronger than the negative (Berk & Anderson, 2000).
Then, as therapist and client are all
alone in numerous therapy sessions, they cannot help but concentrate on each
other’s feelings and attitudes (Greenacre, 1954). Therapists closely attend to
their clients, as did clients’ mother figures. Clients experience
understanding, non-judgmental professionals (Macalpine, 1959) who make no
emotional counter-demands (Greenacre, 1954) and thus seem to love them
unconditionally. At a profoundly deep level, the therapy setting serves as
second womb.
To most clients, regardless of gender,
most therapists come across as having a maternal-nursing attitude toward a
suffering patient-child (Greenacre, 1954). Even when they do not gratify their
clients, they replicate their clients’ early experience of a mother, which is a
combination of gratification and deprivation (Greenson & Wexler, 1969),
with gratification having the greater and longer-lasting effect.
Thus therapy gives clients a perfect
chance to recreate their infantile life in the transference (Bollas, 1983). Experiencing
their therapist as a mother, clients can unconsciously displace their
experiences with their original caregiver (Tower, 1956). They can expect that
their therapist will satisfy all their needs and repair all their injuries
(Horowitz et al, 1984). If only they make themselves appear needy and please
their therapist in a certain way, they can induce their therapist’s care
(Goldin, 1985). Consequently, at first the functioning of the Mother Archetype tends
to be overwhelmingly positive.
It can, however, soon become negative. It
can even become dangerous in the case of clients with pronounced depression,
anxiety, dependency issues, and phobias (Gazzillo et al, 2015) as they and
their therapist resist their mother-child relationship evolving into an
adult-adult relationship. Put succinctly, clients’ journey to independence can rightfully
include an experience of dependence on their therapist, but that dependence
must eventually yield to healthy independence. It must be transitional and
temporary, not overly long-lasting or permanent.
Unfortunately, therapists with unresolved
maternal-child issues are vulnerable to forgetting this. They are prone to
infantilizing their clients and habituating dependence on them. They make
clients who are dependent and want to be cared for regard their therapists as primary change-agents (Chused & Raphling, 1992). In subtle and sundry ways, they
make the mistake of assuring clients that they are not only profoundly
interested in them but also intent on meeting their needs rather than helping them assume that responsibility (Plakun, 1998).
Another danger inherent in the Mother
Archetype is that clients’ expectations of being mothered are often higher than
therapists’ actual performance. Therapists inevitably “mother” imperfectly;
they do not – indeed cannot – fully compensate for clients’ early
experiences of deprivation. Thus therapy can become an occasion of powerful
transferential conflicts within a client and between client and therapist, as
maternal functions promoted by the Mother Archetype supersede key attitudinal
and behavioral variables needed to attain and maintain therapeutic goals.
Gabbard (1996) exposes yet another danger.
Clients with pronounced needs to be mothered can have a strong urge to defend
against the very therapist-client merger they covet. Because they also fear
being “swallowed up” or submerged in the merging process, they withdraw and
become resistive. They even try to seduce their therapist, for they prefer a
sexualized relationship over the threat of losing themselves.
Hence, even if they are spared clients’ seduction
attempts, therapists must never forget that positive outcome depends on how
successfully they balance clients’ need to be “held close” with their need to
be “held separate.” They must give clients “space” in which to become their own
source of nourishment and care. They must promote clients’ self-sufficiency and
autonomy. They must even allow clients to pursue a narcissistic desire to have
“omnipotent” control of them in the course of becoming their own source
of unconditional acceptance and positive regard.
Therapists who unconsciously hold the
belief that they must be benevolent and self-giving to the point of clients getting
from them whatever they want whenever they want it are especially vulnerable to
acting out the Mother Archetype. In the beginning, this enactment appears
benign, even beneficial. Clients benefit from therapists who are
unconditionally empathic and consistently available. In time, however, this
enactment proves malevolent. Therapists eventually grow weary. In the light of
their own self-care needs, they cannot sustain the posture of being always available. Moreover, like all human beings, therapists have an
instinctual sadistic trait against which they cannot endlessly defend (Pick,
1997). It is only a matter of time before they rebel against a system whereby
clients can make endless use of them, forgetting that they themselves have set
it up. Thus they become emotionally abusive of their clients, albeit in very
subtle ways.
Furthermore, it is only a matter of time
before the seemingly positive intimacy engendered by the Mother Archetype
becomes negative enmeshment. Therapists eager to help clients make progress,
for example, might begin by using an educational intervention. Its initial use
is efficacious. But by overusing this intervention ever so slightly, therapists
unwittingly give clients a three-fold message: They know considerably
more than their clients, they can bring about change, their clients
cannot. In time, some therapists begin to do work that clients should
be doing. Thus they permit clients to remain passive, dependent recipients of
care. This is particularly true of clients whose interpersonal style is anaclitic.
For this dependence triggers over-involvement and over-protection in their
therapist (Hennisson, 2019).
For instance, clients stimulate positive
countertransference as they assume the role of a needy child and their
therapists project their need to be a benevolent caregiver. Then, if their
countertransference remains positive, therapists who have introjected and
embellished the role of caregiver unconsciously transform that role into
primary doer or sole source of caregiving. In the end, as clients become
proficient in non-participation – fail to do the homework they agreed to, for
example, or make a habit of asking advice rather than thinking things through
themselves – therapists experience disturbing countertransferential anxiety,
which, in turn, gives rise to negative transference. Then it becomes very
difficult for them to establish and maintain a functioning working alliance
with the client.
Thus because of the Mother Archetype’s
profound influence on the unconscious mind, therapists must maintain a delicate
balance. They must allow clients control over what they do in sessions and
between sessions along with how and when they do it. But they must also require
that clients take primary responsibility for their own growth and development
through age-appropriate, ego-syntonic self-caregiving.
Equally important, therapists must be
neither insistent upon preserving closeness with clients nor determined to
maintain separateness. Despite negative countertransference, they must become
neither silently detached nor intrusive. They will do so if they remember that
their clients’ need to feel secure in therapy because they are being “held” by
their therapist is figurative. They can experience themselves as “children” but
must not be infantilized (Anderson & Przybylinski, 2012). They are in fact
adults (Casement, 1991), or have the potential to be.
At the same time, however, therapists must
keep in mind that carefully selected interventions, such as reflective
listening, can give clients a sense of being held physically that is more real
than if “a real holding … had taken place” (Winnicott, 1988, 61). Their
therapist’s conveying understanding through language will seem to them as if
the therapist were “holding [them] in the past, that is, at the time [they]
needed to be held, the time when love meant physical care and adaptation”
(Winnicott, 1988, 62).
To summarize, the Mother Archetype is by
and large the most relevant archetype in therapy because, like the prototypic
mother-child relationship, therapy involves repeated, intimate contact between
two persons through conscious and unconscious channels of communication (Tower,
1956). Reminiscent of the womb, therapy is a golden opportunity for clients to
find, once more, the vanished mother figure (Ferenczi, 1909). It is a chance to
enjoy again the mother-infant quasi-union of the first months of life
(Greenacre, 1954).
Similarly, therapy becomes an opportunity
for therapists to play maternal roles of creating and nourishing new psychic
life. In the hands of therapists who provide security by “holding” their
clients even as they allow them to “move freely,” the Mother Archetype facilitates
therapeutic progress.
At
the same time, the Mother Archetype can prove dangerous. In the hands of
therapists who do not detect and deal with their clients’ negative transference
and problematic aspects of their positive transference, along with their own
problematic countertransference, the Mother Archetype can moderate therapeutic
progress and mediate treatment failure.
The Father Archetype
The Father Archetype embodies another
essential aspect of human development: morality and its foundation in
authority. 18 The mother might be the chief moral socializer (Badcock, 2009), but the father
represents the conscience, that psychological phenomenon that facilitates doing
what is right and good for others, even if it is personally difficult (Nunberg,
1951), in order to preserve and protect life.
Thus the Father Archetype brings out the
human instinct to sacrifice oneself for the good of the species. It encourages
one to protect and defend life even at the cost of one’s own life.
Consequently, the Father Archetype is a major trigger of transference and
countertransference in therapy.
Freud once said that the death of a man’s
father is the most important event in his life (Reik, 1937). It could hardly be
otherwise for both men and women when that protector and defender of life
departs, never to return.
Clients easily displace conflictual material from their biological father to their therapist, regardless of gender, because in one way or another they want to use therapy to protect or restore their intrapersonal and interpersonal well-being. The problem they begin therapy with has resulted from a violation of conscience, though they rarely describe it in terms of morality.
Therapists easily assume paternal roles
because they see their primary function as preserving or renewing psychological
life. That life, they come to realize, is often a matter of resolving an extremely
detrimental conflict between behavior and moral values. This is especially true
of clients with significant depression and/or anxiety. It is particularly true
of persons whose suicidal ideation correlates with PTSD (Colson et al, 1986)
and with those whose interpersonal style is highly dependent (Hennisson, 2019).
Indeed, the preservation and protection of
life is a matter of members of society living according to a moral code. All
must develop a conscience and abide by its distinction between good and evil.
For most, it is a matter of resolving conscience conflicts: changing oneself
when one’s behavior harms others.
Unfortunately, however, the human
condition often brings out the opposite: not acting morally but expecting
others to do so. Thus clients present with goals of getting others to change.
They also unconsciously want their therapist, not them, to take responsibility
for their goal attainment. Effective therapists, however, help clients realize
that it is they who must change, even to the point of sacrificing what
is dearest to them. Hence, conflicts inherent in the Father Archetype develop
within clients as well as between clients and therapists.
It has long been noted that most
therapists choose their profession because of a deep-seated “savior” complex
(Little, 1951; Cohen, 1952). Thus the Father Archetype appeals to them. They
believe that they are meant to save both themselves and others. In fact, by
introjecting their clients’ Father Archetypal transference, they can save
themselves by saving their clients.
As a consequence, they find it appealing
to establish a paternal-based relationship with their clients (Westen &
Gabbard, 1998). They set a treatment framework, suggest a treatment plan, and
impose certain expectations on their clients. Therapists who unconsciously
believe themselves to be innately omniscient and omnipotent authority figures
are especially vulnerable to enacting the Father Archetype. They believe that
they have the right to dictate morality. If something is wrong for them, it is
wrong for their clients; if right for them, right for their clients. And they
easily adopt a corollary belief: They are absolutely necessary for clients’
progress. Clients need to be rescued, healed, and protected, and they are rescuers, healers, and protectors par excellence.
Ironically, therapists who fail to
recognize their savior complex can even harbor unconscious prohibitions against
their clients’ getting well. It is illness, after all, that makes the
therapist’s presence a necessity.
Danger then arises for at least two
reasons. First, although most clients want to get better on a conscious level,
on an unconscious level many want to remain ill. Their symptoms enable them to
feel connected with an early, omnipotent father figure. They “want to hold onto
[an] imagined perfect, or at least powerful, [person] from their past. [They
desire] to see the therapist as omnipotent rather than face the disappointment
of seeing the real therapist” (Alpert, 1992, 147).
Second,
therapists are especially vulnerable to reparative functions, and clients
become persons to whom therapists wish to make amends (Little, 1951; Pick,
1997). Indeed, repressed desires to rescue and perform reparative functions are
the very basis of countertransference in the therapeutic setting (Volkan,
1995). When therapists hear about – indeed share – their clients’ pain, they want
to restore them to a pain-free emotional life. If clients let themselves be
restored, all is well. If not, therapists become increasingly anxious, which,
in turn, increases their desire to heal. And the vicious cycle begins again. 19
Particularly vulnerable to the negative
side of the Father Archetype are therapists who have had a depressed mother.
Unless they have done considerable personal work, their depressed mother, be
she alive or deceased, continues to induce rescue and reparative fantasies
(Racker, 1972).
While on the surface this need would seem
to be positive or at least harmless, it inevitably becomes harmful for several
reasons. First, reparative needs easily become reparative impulses, which, in
turn become compulsions (Little, 1951). Therapists unconsciously keep
clients impaired because they want to make them well again and again.
Second, therapists’ reparative needs cause
them to unconsciously identify with clients’ unconscious prohibitions against
getting better that stem from their primitive aggressive instincts. Thus as
clients express their early aggressive tendencies by thwarting therapists’
efforts, therapists unwittingly exploit clients’ sickness for what it does for them (Little, 1951).
Third, therapists’ reparative needs impede
clients’ movement from being a victim to whom reparation is due to a
person who does what it takes to survive. This includes rejecting powerful
reinforcement from self-pity and special attention from others.
All this is not to deny the beneficial
potential of the Father Archetype. In the hands of therapists who foster
conscience development, personal responsibility, and self-protection from
avoidable or renounceable emotional pain, the Father Archetype mediates and/or
moderates positive therapeutic outcomes.
The Sibling Rivalry Archetype
Jung’s (1966) Sibling Rivalry Archetype triggers transference because it promotes expectations of getting one’s way, winning over competitors, and placating others if victory is not within reach. Though clients might see therapists as parents when they begin therapy, as therapists reveal their shortcomings, clients begin to regard them as mere siblings competing for some obscure prize or preferred place in the family. This can also happen when clients with histrionic or psychopathic traits find out that therapists have other clients (Ferenczi, 1909; Gazzillo et al, 2015; Tummala-Narra, 2019).
The Sibling Rivalry Archetype evokes clients’ need for psychological space that allows them to become themselves, different from their siblings while still belonging to a family. This extends to becoming different from their therapist, who is another sibling.
The Sibling Rivalry Archetype also evokes clients’ need to make therapeutic progress as soon as possible for the sake of becoming a formidable competitor. However, clients tend to define progress in terms of relief from the pain that brought them into therapy rather than acknowledging their own contribution to that pain. They typically want to address relatively superficial material. They want others to change. And they want their therapist to fix their problems and to do so quickly. Thus they will not have to hold themselves responsible for making difficult changes in how they think and behave (Schafer, 1997).
Therapists with unresolved conflicts regarding being liked by their clients because they assume responsibility for fixing their problems and not being liked because they assign their clients primary responsibility for change are especially vulnerable to the Sibling Rivalry Archetype. They tend to compete with clients by working harder than clients to attain treatment goals. They give into being not only resourceful persons but also older “siblings” that can be used to the point of being abused. They let what is basically appropriate in therapy, namely facilitating problem solution, become taking primary responsibility for it. Therapeutic progress depends much more on them than their clients.
On an unconscious level, these therapists also make the therapy constellation a virtual family in which they compete with those who are outside of therapy for being of greatest help to clients. They want their clients to make them the main focus of their internal world. Clients are to follow the lead of their therapists. Family members are not to interfere.
In other words, clients are to move from responding positively to the help they get to being indebted and grateful to their therapist for all that is done for them.. Then, to the extent that their clients express gratitude, these therapists can fall into the insidious trap of meeting their affiliative needs, primarily or solely, through their work. They may go as far as to unconsciously encourage erotic feelings in clients. For instance, they may ask for unnecessary details of clients’ sexual fantasies (Gabbard, 1996) for their own gratification.
Similarly, these therapists may unconsciously encourage clients’ erotic fantasies about them, only to become cold and aloof in response to clients’ longings. They may give clients the message that sexual feelings are unacceptable, even disgusting. Unfortunately, this may confirm clients’ own beliefs. Caught in the compulsiveness characteristic of transference, clients may then re-enact prior victimization (Schafer, 1997).
Even if therapists do not engage in boundary violations, if the Sibling Rivalry Archetype is not properly addressed, competition between client and therapist can occur in key areas like goal attainment. Therapists can demand that clients change, whereupon clients rebel by resisting the work that entails. Or they terminate therapy (Ogden, 1994) and thus win the competition of just who is in charge of their lives. Alternately, they comply with their therapist’s demands outwardly and for the time being, enjoying all the while that they are the winners of the competition.
Put succinctly, the Sibling Rivalry Archetype challenges therapists to deal with their clients’ and their own proclivity to compete rather than collaborate, to vie for resources rather than share them, to get their way rather than compromise, and to win over others rather than with them.
The God and Goddess Archetypes
The God and Goddess Archetypes trigger
transference and countertransference in therapy because of the developmental
need for autonomy (Jung, 1966). They promote twin fantasies of omnipotent
control and self-sufficiency (Klein, 1957). They nurture authority-based
illusions of being smart enough to outwit “the gods” and powerful enough to
rectify wrongs by punishing and rewarding others.
The God and Goddess Archetypes are especially influential in therapy because of clients’ feelings of inferiority and their belief in their therapist’s superiority (Gabbard, 1996). Especially for clients with depressed/depleted narcissistic disorders and paranoia (Gazzillo et al, 2015), therapists’ ability to use therapeutic interventions can serve as a painful reminder of others’ superior creative powers and their own inferiority (Epstein, 1977). In fact, envy is aroused in some clients principally by their therapist’s interpretative ability (Klein. 1957). Ironically, while therapists only want to facilitate insight by interpreting, doing so can be a therapeutic mistake. 20
He was an
attractive but needy client who had just been jilted in love. However, he was
also seducing a vulnerable married woman. When the woman finally decided to end
their emotional affair, he was so furious he vowed to reveal the affair to
her husband. He would hear of nothing else.
His therapist
wondered whether she should simply reflect her client’s feelings or share her
countertransferential anger triggered by his total disregard for the harm he
was doing to a third party.
She chose the latter, only to have her client terminate therapy. He would not take personal responsibility for what he had done and planned to do. He was a god above reproach. He had the right to punish others. He would mitigate his loss by experiencing his “omnipotence.”
In hindsight, the therapist realized that she should have continued to make intrapersonal diagnostic use of her client’s transference rather than share her countertransference. She would then have learned experientially why her client was resentful of suggestions that he focus on his personal responsibility, found it so painful to do so, and just could not do so at the time. Once those reasons were addressed, he might have been able to reduce his defensiveness and explore his fear of taking responsibility for his actions. He may never have assumed that responsibility, but premature termination eliminated even that possibility.
Instead, the God and Goddess Archetypes set the stage for an unsuccessful outcome in spite of a well-intentioned therapist and an ordinarily efficacious intervention. She needed to address her own goddess issues: her assuming that she had power over her client and the right to highjack the therapeutic process.
21
It would have been wiser for her to focus on the power struggle they were in due to the operation of the God and Goddess Archetypes. They both unconsciously wanted to escape their emotional pain by controlling the therapeutic process (Schafer, 1997). She wanted to escape her feelings of powerlessness by asserting godlike authority over a vulnerable client. Her client wanted to transfer his anger toward the woman who rejected him to his therapist. He would thereby enjoy the illusion of outwitting and punishing his therapist. He would get relief from being under her godlike control by assuming his own godlike authority. It would be an amazingly powerful, though illusory, experience (Grinberg, 1997) of healing his affiliative pain.
Clients and therapists who experience
failure of the parental holding environment are especially inclined to embrace
the God and Goddess Archetypes. Because they have had to sustain and nourish
themselves, they instinctively adopt the schema of being omnipotently self-sufficient
(Modell, 1980). They even believe that they must parent their therapist or
client, much as they once did their parents. In doing so, they will gain power
over them.
Paradoxically,
fear of being personally omnipotent is also embedded in the God and Goddess
Archetypes. Thus clients and therapists fear the unending power and authority
which that state conveys and, even more so, not being able to find
well-modulated support: an equal or at least a powerful companion-other (Stein,
1993).
At
the same time, they fear domination and absolute control by that companion
because they associate overt power with eventual covert enslavement. They fear
having put themselves at risk for being exploited (Modell, 1980).
Therapists who hold the unconscious belief
that they are superior to others because of their education, experience, and
professional success are especially vulnerable to enacting the God and Goddess
Archetypes. They assume that they are extraordinarily gifted. That they are
remarkably skillful in their perception, analytic and synthesis abilities,
instinct, and ability to deal effectively with affect. Some even believe they
are magical.
Because they actually have a certain
amount of a priori knowledge due to their experience and education, they
succumb to fantasies of having innate power and authority (Bion, 1967) in the
therapeutic setting. When, in addition, clients transfer to them their
culturally-encouraged reverence and awe for professionals called “doctor,” they
are tempted to believe that they are superior to their clients, even
superior to people in general (Cohen, 1952). Unsuspected and unacknowledged in
the unconscious, this countertransferential force becomes a “recipe” for
ultimate therapeutic failure.
The God and Goddess Archetypes also
inspire fantasies of an ideal world with which therapists unconsciously
identify (Racker, 1972). Their deductions are the truth. They are
offended and shamed when clients challenge them and, most likely, project their
own shame. Thus they become depressed 22 and let other things, like poor evaluations, increase their fear of their
“incompetence” being disclosed. In return, they attribute treatment failure entirely
to clients.
They also adopt the belief that
therapeutic failures cannot and will not be tolerated. Although they do not
consciously deny that mistakes are part of being human, they unconsciously
regard possible failure as a reason to defend themselves against what would
otherwise be wholesome feedback. Thus they fail to learn the lessons that
therapeutic mistakes teach and, in the end, increase the probability of future
failures.
Unfortunately,
in response to therapists’ fear of professional failure, clients tend to develop
even stronger resistance to working with them. They even begin to hate their
therapists (Blum, 1997), which, in turn, makes therapists with omnipotent
self-beliefs dislike, even hate, both themselves and their clients. 23 They may even wish to attack or annihilate the clients they hate and, finding
this unacceptable, project it onto their clients. When clients, especially
adolescents, receive this projective identification, the worst proves true.
They engage in self-destructive behaviors24 or activities dangerous to others (Ogden, 1994).
The therapist
thought that he liked his adolescent client despite the therapeutic
challenges she was providing. Besides not going to school, she was running away
from home and using drugs. He reflected often on how he thought that he really
listened to her; in fact, he listened and listened and listened, then responded
empathically. He seldom challenged her, and when he did so, he was respectful
and gentle. Yet his client continued her self-destructive behavior.
“Can I continue to
like this client?” the therapist began to wonder. “I want to so badly that
perhaps I am fooling myself. Maybe that is why my client periodically refers to
parents who can hardly stand her.”
Finally, the
therapist had to admit that the time and energy he was spending on helping
someone change who apparently would not change might be leading to more
negative countertransference than he wanted to admit. He decided to share that
thought, hoping to help his client.
“I find your
behavior so frustrating,” he said. “No matter what we plan and what you say you
will do, you hardly ever do it. Maybe my negativity is something you sense.
Maybe you won’t change because you sense that I don’t like what you are doing
and therefore don’t like you.”
The client
listened attentively but said nothing. At the end of the session, however, she
referred to no one really wanting her, not even her parents. Listening
intently, the therapist held his client’s pain. And he held it in subsequent
sessions until, when it finally lost its grip on her, she no longer had to act
out.
As this vignette reveals, therapists’ denial of unpleasant truths about themselves as they enact the God and Goddess Archetypes can weaken, if not destroy, the therapeutic and working alliances. Contrastingly, by acknowledging their negative countertransference, therapists can empower clients to acknowledge their own deep pain.
Another way therapists enact the God and Goddess Archetypes is by engaging in manic interpretive activity as a way of controlling depressive anxiety related to feelings of clinical impotence (Epstein, 1977). This tends to be the case when clients are medical, legal, and other highly respected professionals. But manic activity only makes matters worse. It is one thing for therapists to periodically direct the therapeutic process. It is another for them to maintain control of it.
One reason is that clients tend to be ambivalent both about the therapeutic bond (Fox, 1998) and about the power and authority they presume their therapists have. They both love and hate their therapists. They both idealize them and depreciate them (Olinick, 1996
). They want to receive their attention but deny their authority (Freud, 1915). Paradoxically, they desire to surrender to their therapist’s authority – even turn over self-responsibility – but stay in control. If clients actually surrender, sooner or later they rebel and demand that their all-benevolent, all-powerful therapist return power to them. It is not to be a matter of returning
responsibility to them
, however. For they want to do what they want without facing consequences. Indeed, clients’ refusal to take responsibility for their life is even more pervasive than their wanting constant reassurance that they can do so (Schafer, 1997).
25
A second reason therapists’ maintaining control of therapeutic work backfires is that it leads to their responding negatively when therapeutic success is minimal or non-existent. It allows them to express their anger in ways that feel good at the time: to covertly punish their clients, to get subtle revenge, to engage in imperceptible payback. It even allows them to justify hating their clients. Of course, therapists consciously try to keep these feelings from clients. Unconsciously, however, they act them out. Thus clients experience countertransferential maltreatment, which leads to therapeutic stalemates and failures (Blum, 1997). 26
Finally, some therapists enact the God and
Goddess Archetypes by unconsciously believing that they can use any available
therapeutic measure, even sexual involvement with clients, to ensure
therapeutic success (Searles, 1975).
In sum, undetected and unaddressed God and
Goddess Archetypal phenomena are exceedingly dangerous. Therapists’ and
clients’ fantasies of omnipotence are major obstacles to effective therapy
(Bion, 1967). We have “the urge to deification of the other, the constant
placing of certain select persons on pedestals, the reading into them of extra
powers [for] the more they have, the more rubs off on us,” writes Becker (1973,
148). And, “thanks” to the God and Goddess Archetype, often “the other” is
actually our ideal self.
Thus therapists’ responsibility to reckon
with the God and Goddess Archetypes. They and their clients might, for example,
translate god and goddess into hero and heroine whose
integrity and courage can be imitated (Becker, 1973). In the end, both
individuals and society might then benefit from what cannot be eradicated: the
influence of the God and Goddess Archetypes.
The Animus and Anima Archetypes
Jung’s Animus and Anima Archetypes trigger
transference and countertransference in therapy because both therapists and
clients hold profound, unconscious expectations of completion. They want to
become whole persons. They want to add the strengths of another person to their
own. They are “always trying to deliver [themselves] into the power of a
partner who seems compounded of all the qualities [they] have failed to realize
in [themselves]” (Jung, 1969, 156).
Strictly speaking, the Animus and Anima
Archetypes refer to the strengths of the masculine and feminine sex. In
contemporary usage, however, they refer to gender or one’s perception of having
a masculine or feminine orientation.
The animus, an archetype within the female
psyche, is “the deposit … of all men’s ancestral experiences of woman” (Jung,
1966, 209). The anima, a comparable archetype within the male psyche, is a
detailed outline of women’s ancestral experiences of men. Men are compensated
by a feminine element, as women are by a masculine element as both genders
search for wholeness, completeness, and unity. Both men and women achieve
strength and power through attachment to what they are not (Jung, 1966).
The animus brings with him the logical and
the cognitive, especially the ability to discriminate (Jung, 1966). If
transference and countertransference become fully operative, the animus,
partial as he is to argument, can be seen at work in women, in disputes wherein
they have an unshakable feeling of rightness and righteousness. Of course, “men
can argue in a very womanish way, too, when they are anima-possessed and have
thus been transformed into the animus of their own anima” (Jung, 1966, 153).
With women, the argument soon becomes a
matter of personal vanity and touchiness rather than content. With men, the
argument soon becomes a matter of power, be it truth or justice or some other
“ism.” Their dialogue becomes marked by misapplied truisms, cliches,
platitudes, opinionated views, insinuations, misconstructions, and
misinterpretations. 27 Nothing is important except proving one’s point, with the result that the
therapeutic alliance can be seriously weakened, even destroyed.
Granted that most therapists manage the
animus well enough to resist falling into an obvious argument, they can be righteous
and judgmental in their interpretations. They can be set on having the last
word. They can be overly sensitive to clients’ rejection of their ideas. Their
clients, in turn, tend to reject whatever their therapist says for the
sake of being right.
For her part, the anima brings with her
the relational and emotional, especially the connectedness so needed in
interpersonal relationships (Jung, 1966). Thus she can become a source of
life-giving energy. She can help both men and women learn to accept in
themselves and each other a partly positive, partly negative self-image. Thus
they can enjoy elemental, feminine dynamism (Ulanov, 1984).
On the other hand, the anima can make both
men and women highly alert to each other’s shortcomings and reluctant to
explore their own contribution to problematic relationships. Wanting to
maintain an exaggeratedly positive self-image, clients and therapists can
consciously collaborate, yet unconsciously resist, honest interpersonal
evaluation. They can become offended at the implication of personal weakness.
They can abort fruitful evaluation by retaliating in passive-aggressive ways.
In sum, the Animus and Anima Archetypes can
mediate significant wholeness and completeness in individuals. They can mediate
openness to the contributions each gender has to the truth that needs to be
discovered and the wisdom that needs to be acquired for family systems
and society to be wholesomely unified.
At the same time, the Animus and Anima
Archetypes can ruin therapy by bringing out the worst in clients and
therapists, regardless of gender. They can mediate despicable behavior, both
verbal and non-verbal, that brings therapy to a disastrous end.
Final Thoughts
First, it is more than clear that all the
archetypes are double-edged swords: benevolent or malevolent. It all depends on
what therapists do with transferential and countertransferential material they
trigger.
Second, in light of the potential of the archetypes to wreak havoc in interpersonal relationships, it is crucial for therapists from cultures that differ from those of their clients to discover ways in which specific archetypes might be impacting their interactions. They must detect transference and countertransference phenomena (Mishne, 2003) as early as possible so that they can help their clients “become aware of, review, and alter obsolete conclusions that determine their contemporary approaches to their lives” (Renik, 1990, 199).
They can then also collaborate with their clients to resolve personal, interpersonal, and cultural conflicts that lie beneath various human needs and otherwise lead to unending aggression. Neither therapists nor clients can deny those needs, for they are universal and integral to psychological functioning. But they can learn appropriate ways of meeting them.
Footnotes
(
Note: To return to the course after having clicked a footnote, click the Back button in your browser.)
Note 1. Some theorists, like Meissner
(1966), hold that “projection … creates pressure in the interpersonal
interaction to draw the other member of that interaction to fulfill the
expectations and inherent demands of the projection.” I prefer to make a
distinction between projection and projective identification, wherein only the
latter creates the pressure. See the next section for a more
detailed explanation. (Go back)
Note 2. See my
book Transference and
Countertransference in Non-Analytic Therapy: Double-Edged Swords. (Lanham, MD: University Press of America, 2007) for a more thorough explanation
derived from recent research.
Note 3. Therapists
must learn to identify the conflictual wishes, urges, and fears originating in
a very early time that energize clients to perceive something in the present.
They can then help clients subject these phenomena to reality testing.
Note 4. Clinical experience also led Freudian theorists to regard transference as a blend of positive and negative elements. Sooner or later, transference that appeared to be positive revealed its conflictual basis. Clients might perceive their therapist as a protective father, for example, but eventually notice that he does not protect them from all pain. By contrast, transference that appears to be negative eventually showed its positive aspects. If clients could be helped to express their negative transferential emotions and to experience their therapists as non-retaliatory as they drew attention to the transference, they could discover the positive affect under the negative transference. Hatred of the therapist who fell short in providing protection, for example, usually cloaked longing for and love of the parent who was projected onto the therapist.
Note 5. Influenced
by this thinking, many late-20th century theorists put major
emphasis on here-and-now transference enactments during therapy (Kernberg,
1987; Binder, 1996). They advise therapists to interpret what is happening in
the session at hand (Danvanloo, 1978; Malan, 1976b; Sifneos, 1979; Luborsky,
1984; Strupp & Binder, 1984). They hold that, although therapists can
obtain information about clients’ interpersonal history, they do not have to
include that data in their interpretations (Malan, 1976a). Their first priority
is to help clients understand that although their problems probably began in
early child-parent experiences, they need to address the current situation
rather than its past origins. Indeed, many contemporary clinicians who think of
transference in a totalistic sense prefer not to make distinctions between past
and present conflictual material. They see it as virtually impossible to tease them apart.. Are clients angry simply because their therapist is criticizing them? Or are they angrier than usual because they experience that criticism as similar to that of their teachers, adding injury to injury? Asking clients may be helpful for those who are particularly insightful may have vague suspicions, but clients’ powerful emotions are likely to obstruct clear associations.
Note 6. Searles (1975) has given another explanation for clients’ transferential re-enactment: clients are unconsciously attempting to contribute to their therapists’ own emotional growth, integration, and maturation. Clients are giving their therapists an opportunity to resolve their own conflicts. Instinctively realizing that their own growth and integration depend heavily on that of significant others, clients surmise that unless their therapists become mature, their own maturity will be weakened. At the same time, clients unconsciously want significant others to change so that they do not have to make personal changes themselves. They have identified with long-lived immature emotional states and dysfunctional relational patterns to the extent that changing themselves feels like losing themselves. In addition, clients want to be mature without suffering the pain of personal change. The solution? Becoming mature by relating to a therapist who has become mature in the course of resolving the conflicts that they, as clients, have introduced into the therapeutic setting. Of course, this will work only if transference and countertransference are dealt with consciously.
Note 7. Attempts to heal simply by enacting transference miscarry in the end because they do not involve any real integrative processing (Ferenczi, 1909). Rather than requiring clients to subject distortions to rational scrutiny and thereby change the nature of similar present relationships, transference – in and of itself – allows them to enact past relationships with all their distorted attributions and illusions (Freud, 1940). For example, clients may enact a parent-child relationship with their therapist, attributing to themselves an inability to care for themselves and to their therapist the resourcefulness to meet their needs. They fail to take into consideration their own potential for self-nurturance or their therapists’ perceptions of them as resourceful adults. Consequently, these clients cannot integrate a capability for self-nurturance into their psyche. They remain conflicted over others’ refusal to meet that need, leaving their present relationships no healthier than their past.
Thus therapists must help clients “determine where … self-images and [interpersonal] patterns came from, how they may have been adaptive at the time they were initiated, and whether they are still adaptive or are self-defeating and maladaptive and therefore need to be changed” (Bollas, 1987, 3). Through transference-focused therapy, clients will see what they are doing to avoid pain – indeed they will run smack into the pain – and finally, by dealing with it, discover from experience that they can face it and survive. Thus identifying and dealing with transference becomes the primary means by which clients reduce, if not completely eliminate, their historical and potential psychic pain (Lear, 1993).
Note 8. Transference can reveal itself anywhere along a continuum from simple or fragmentary thoughts to elaborate schema or scripts that give meaning to repressed experience. “This particular therapist resembles another person with whom I should have felt good,” clients might unconsciously “think.” Alternately, clients might use “Buxom, smiling women are mother figures who will make up for the nurturing I never got” as a schema whereby they classify everyone with those features as maternal.
Note 9. “Transference and
countertransference sometimes occur without a transference-countertransference
interaction” (Meissner, 1996, 307). However, the view of countertransference as
inherently interactive has become increasingly accepted (Gabbard, 1994).
Note 10. Therapists unconsciously
introject what is given them: “messages about roles, functions,
self-definitions, and traits.” Because these “messages” are given repeatedly,
therapists “hear” them, “read” them, and take them to heart on an emotional
level without being conscious of what they are doing. In other
words, introjection is ever present as a companion to projection.
Note 11. There is an element of reality in
that those being given a projection have some of the objectionable attribute or
at least the potential to act in the objectionable way (Searles, 1975).
Note 12. We go on to believe leaders who
warn us that migrants to our country are terrorists. We must be on our guard
lest they enter our country. We perpetuate fear of our own
death. We do not resolve the conflict over wanting to deny our immortality and
realizing that we cannot win over death (Becker, 1973).
Note 13. For instance, therapists might experience frustration because of their “good client” template when clients say little or nothing even though they came on time. However, therapists are also being influenced by their clients’ unconscious need to punish them for exacting promptness from them, as did their parents, no matter the cost to them. Clients’ present behavior is a manifestation of clients’ transference as well as the countertransferential communication they have received from their therapists.
Note
14. Thus the traits are not the same as they were originally because the recipients have contained and managed them in their own unique ways without even being aware of them. Under most circumstances, the recipients have lived with the undesirable traits without having “allowed” them to damage other aspects of the self, (Little, 1957). Ironically, if the traits were not totally ego-dystonic to recipients, in some way the recipients may have even enjoyed them. Controlling people who need control, for example, can feel pleasant to those who control.
When the recipients are criticized for the traits, however, they find what has happened problematic. To the extent that there is a “kernel of truth” in their having at least some aspects of the unwanted traits, they become defensive. They are caught between becoming aware of painful feelings related to the - traits and denying them.
Note
15. Therapists must remember that it is not only clients who engage in projective identification. They do so themselves. For instance, they project their fantasy of omnipotence, which is easily transferred from an earlier narcissistic period of development; assign their clients the role of patients healed at the hands of their therapists; and then pressure their clients to be “cured.” Thus therapists must process their projective identifications no less than help their clients to do so.
Note 16. Winnicott (1965) regards the fact
that therapists bring their own unresolved conflicts to bear upon the therapy
situation as unrealistic, even abnormal. It is both abnormal and unrealistic,
for example, to desire to be exacting with an older woman client simply because
she is like women teachers who were exacting with the therapist in the past.
What would be normal and realistic, by contrast, would be the same therapist’s
urge to hold the older woman client strictly accountable for being prompt for
her sessions, as the therapist does all clients. The client’s promptness
ensures income each week, additional income from the next client, and the
therapist’s sense of accomplishment, all of which reflect the therapist’s work
ethic and personality.
Note 17. The abuse that certain
clients suffered presents special difficulties, for within the psychic
structure of many victims lies a figure who is, paradoxically, both a protector
and a persecutor image (Kalsched, 1996).
Note 18. Would a fundamentalist culture have a special impact in the case of the Father Archetype?
Note 19. These therapists consciously
conclude that failing with a client is more than a personal problem
(Sharpe, 1930). It means that clients will not get better, and therapists will
be failures.
Note 20. It is not unusual for clients to harbor a deep, passive wish to defeat the therapists that they love when they realize that therapists are much more resourceful and insightful than they are. “You are so great, my fate lies in your hands; do your best and I shall yet defeat you” (Stein, 1981), clients unwittingly warn as envy surfaces. Like other envious persons, clients try to defeat envied others rather than acquire their skills.
Note 21. What might be the impact of
therapists belonging to a majority culture and clients belonging to a
minority culture? Of white privilege in the case of an African-American client?
Of gender in a patriarchal institution?
Note 22. What might be the impact of some
Asian cultures that regard shame as unacceptable to oneself?
Note 23. Blum (1997) believes that transference hate can become an even greater problem than transference love because it reaches even deeper into clients’ and therapists’ psyches than does their loving. It threatens their fundamental self-esteem. Nevertheless, transference hate and countertransference hate are easily repressed or denied because they seem contrary to the therapeutic alliance. “Clients should not hate their attentive therapists, and therapists should not hate their vulnerable clients,” cultural and psychotherapeutic traditions hold. If hate is present, it must be denied. Then, like other denied and repressed emotions, hate intensifies on an unconscious level even as it is minimized on a conscious level. As a result, hate can be unwittingly enacted by clients, and even by therapists. In turn, enactments of hate are powerfully reinforced by resultant experiences of self-enhancing power and enjoyable vindication.
Hate tends to be strong when intimacy fears surface. However desperately clients want to be in a close, loving relationship, few have learned to tolerate the stress of intimacy. When it surfaces and therapists do not draw attention to it, clients often resort to such hate-based maneuvers as reducing the effectiveness of their therapist. They induce guilt in them, especially those who need to be needed, by acting-out and thereby destroying any plan to improve (Herron & Rouslin, 1982).
Note 24. Perhaps nothing causes greater transferential conflict than suicidal desires of clients and the anti-suicide stance of therapists, for the possibility of clients committing suicide reminds therapists of losses they had to accept in their families of origin. Hence, therapists experience conflict over holding and containing their clients’ suicidal desires and wanting to eradicate them as soon as possible. In turn, therapists’ inability to resolve these conflicts satisfactorily can result in loss of rapport or even loss of the therapeutic alliance.
Note 25. Conflicts arise in therapy as therapists attempt to determine how and when to interpret clients’ refusal to take responsibility for their lives and their therapy. Working most obviously within the God and Goddess Archetype, therapists must balance their need to be ultimately responsible for the therapeutic process with their clients’ need to take responsibility for their own lives, including their therapeutic “life.”
Note 26. Therapists must resolve the thorny conflict of accepting their clients as they are while challenging them to grow in maturity and responsibility. Therapists must come to a satisfactory balance between respecting clients’ perspectives and questioning the distortions they harbor (Handley, 1995).
Note 27. What might be the impact of
American political affiliations in an election year?
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders, (5th edition). Author.
Alpert, M. C. (1992). Accelerated empathic therapy: A new short-term dynamic psychotherapy. International Journal of Short-Term Psychotherapy, 7, 133-156.
Amid, B., Aron, L., & Bachar, E. (2020). Selfless self-transcendence in the clinical setting as a source of self-enhancement. American Journal of Psychoanalysis, 80, 16-36.
Andersen, S., & Przybylinski, E. (2012). Experiments on transference in interpersonal relations: Implications for treatment. Psychotherapy, 49, 370-383.
Atlas, G., & Aron, L. (2018). Dramatic dialogue: Contemporary clinical practice. Routledge.
Bach, S. (2019). The inner world, the gut, and the sense of reality. Psychoanalytic Psychology. Advance online publication. http://dx,doi.org/10.1037/pap0000256.
Bachant, J., & Adler, D. (1997). Transference: Co-constructed or brought to the interaction? Journal of the American Psychoanalytic Association, 45, 1097-1120.
Badcock, C. (2009). The imprinted brain: How genes set the balance of the mind between autism and psychosis. Jessica Kinsley Publishers.
Becker, E. (1973). The denial of death. The Free Press.
Benedek, T. (1953). Dynamics of the countertransference. Bulletin of the Menninger Clinic, 17, 201-208.
Berk, M., & Anderson, S. (2000). The impact of past relationships on interpersonal behavior: Behavioral confirmation in the social-cognitive process of transference. Journal of Personality and Social Psychology, 79, 546-562.
Bion, W. R. (1967). Notes on memory and desires. Psychoanalytic Forum, 2, 272-273 and 279-280.
Blum, H. P. (1986a). Countertransference and the theory of technique: Discussion. Journal of the American Psychoanalytic Association, 34, 309-328.
Blum, H. P. (1997). Clinical and developmental dimensions of hate. Journal of the American Psychoanalytic Association, 45(2), 359-375.
Bollas, C. (1983). Expressive use of the countertransference. Contemporary Psychoanalysis, 19, 1-34.
Bollas, C. (19887). The shadow of the object: Psychoanalysis of the unthought known. Free Association Books.
Bowlby, J. (1982). Attachment. NY: Basic Books, Inc.
Brenner, C. (1976). Psychoanalytic technique and psychic conflict. International Universities Press.
Brodbeck, H. (1995). The psychoanalyst as participant and observer in the psychoanalytic process: Some thoughts on countertransference from a constructionist perspective. Psychoanalysis and Contemporary Thought, 18, 531-558.
Carsky, M., & Chardavoyne, J. (2017). Transference focused psychotherapy and the language of action. Psychoanalytic Psychology, 34, 397-403.
Casement, P. (1991). Learning from the patient. The Guilford Press.
Chodorow, N. (1978). The reproduction of mothering: Psychoanalysis and the sociology of gender. University of California Press.
Chodorow, N. (1996). Reflections on the authority of the past in psychoanalytic thinking. Psychoanalytic Quarterly, 65, 32-51.
Churchill, H., & Ridenour, J. (2019). Coming together through falling apart: Using psychological assessment within a developmental framework to assess change. Rorschachiana, 40, 151-168.
Chused J., & Raphling, C. (1992). The analyst’s mistakes. Journal of the American Psychoanalytic Association, 40, 137-149.
Cohen, M. B. (1952). Countertransference and anxiety. Psychiatry, 15, 231-243.
Colli, A., Gagliardini, G., Degl’Innocenti, B., Monti, M., & Foresti, G. (2019). What psychoanalysts do in their everyday clinical practice: Empirically derived prototypes of the psychoanalytic process. Psychoanalytic Psychology. http://.doi.org/10.1037/pap0000231
Colli, A., Tanzilli, Al, Dimaggio, G., & Lingiardi, V. (2012). Patient personality and therapist response: An empirical investigation. The American Journal of Psychiatry, 171, 102-108.
Colson, C., Allen, J., Coyne, L., Dexter, N., Jehl, N., Mayer, C., & Spohn, H. (1986). An anatomy of countertransference: Staff reactions to difficult psychiatric hospital patients. Hospital and Community Psychiatry, 37, 923-928.
Comas-Diaz, L., & Jacobsen, F.M. (1991). Ethnocultural transference and countertransference in the therapeutic dyad. American Journal of Orthopsychiatry, 61, 392-402.
Cooper, A. M. (1987). Changes in psychoanalytical ideas: Transference interpretation. Journal of the American Psychoanalytical Association, 35, 77-98.
Davids, J. (2022). Hot feelings: sexual transference and countertransference with male mid-adolescents and a female psychoanalyst. The Psychoanalytic Quarterly, 91, 709-735.
Davies, J. M., & Frawley, M. G. (1994). Treating the adult survivor of childhood sexual abuse: A Psychoanalytic perspective. Basic Books.
Davies, J. M., & Frawley, M. G. (1992). Dissociative processes and transference-countertransference paradigms in the psychoanalytically oriented treatment of adult survivors of childhood sexual abuse. Psychoanalytic Dialogues, 2(1), 5–36. https://doi.org/10.1080/10481889209538920
DeLaCour, E. P. (1985). Aspects of transference interpretation. Smith College Studies in Social Work, 56, 1-14.
Deutsch, H. (1926). Occult processes during psychoanalysis. In G. Devereux (Ed.), Psychoanalysis and the occult (pp.133-146). International Universities Press.
Dewald, P. A. (1994). The supportive and active psychotherapies. Jason Aronson, Inc.
Ecker, B., & Hulley, L. (1996). Brief-oriented depth therapy. Jossey-Bass.
Egan, S. (2022). From pain to purpose: A psychodynamically and psychosocially informed narrative inquiry into suicide bereavement. Dissertation: University of the West of England. UK.
Egan, S. K., & Perry, D. (2001). Gender identity: A multidimensional analysis with implications for psychosocial adjustment. Developmental Psychology, 37, 451-463.
Epstein, L. (1977). The therapeutic function of hate in the countertransference. Contemporary Psychoanalysis, 13, 442-461.
Ferenczi, S. (1909). Sex in psychoanalysis. Basic Books.
Fleischer, L. (2023). Sandor Ferenczi, the Budapest School of psychanalysis, and the Ferenczi tradition: The bridge between the ‘one-person’ and ‘two-person’ psychology. In B. Huppertz (Ed.).Underlying assumptions in psychoanalytic schools: A comparative perspective (pp. 80-91). Routledge.
Fortuna, T. (2023). In B. Huppertz (Ed.).
Underlying assumptions in psychoanalytic schools: A comparative perspective (pp. 56-69). Routledge.
Fox, R. (1998). The “unobjectionable” positive countertransference. Journal of the American Psychoanalytic Association, 46, 1067-1087.
Franch, N. (1996). Transference and countertransference in the analysis of a child with autistic nuclei. International Journal of Psycho-Analysis, 77, 773-786.
Freud, S. (1900). The interpretation of dreams. Standard Edition, 5. Hogarth Press.
Freud, S. (1910). The future prospects of psychoanalytic therapy. Standard Edition, 11: 141-151. Hogarth Press.
Freud, S. (1912). The dynamics of transference. Standard Edition, 12: 99-108. Hogarth Press.
Freud, S. (1915). Observations on transference-love. Standard Edition, 12: 157-171. Hogarth Press.
Freud, S. (1917). Introductory lectures on psychoanalysis. Standard Edition, 16: 317-326. Hogarth Press.
Freud, S. (1940). An outline of psychoanalysis. Standard Edition, 23: 139-207. Hogarth Press.
Furlong, A. (2022). Establishing and maintaining a therapeutic frame. The Scandinavian Review, 47, 17-25.
Gabbard, G. O. (1994). Sexual excitement and countertransference love in the analyst. Journal of the American Psychoanalytic Association, 42, 1083-1106.
Gabbard, G. O. (1996). Therapeutic approaches to erotic transference. In F. Flack (Ed.), The Hatherleigh guide to psychotherapy (pp. 231-247). Hatherleigh Press.
Gabbard, G. O. (2001). What can neuroscience teach us about transference? Canadian Journal of Psychoanalysis, 9 (1), 1-18.
Gazzillo F., Curtis, J., Bush, M., & Dazzi, N. (2019) Patients’ unconscious testing activity in psychotherapy: A theoretical and empirical overview. Psychoanalytic Psychology, 36, 173-183.
Gelso, J., & Bhatia, A. (2012). Crossing theoretical lines: The role and effect of transference in nonanalytic psychotherapies. Psychotherapy, 49, 384-390.
Gelso, C. J., & Hayes, J. A. (1998). The psychotherapy relationship. John Wiley & Sons, Inc.
Gelso, C., & Hayes, J. (2007). Countertransference and the therapist’s inner experience. Perils and possibilities. Erlbaum.
Ghafouri, S., Summers, F., Dehghani, M., & Shahboulaghi, F. (2019). Process of object relation therapy based on transference and potential space in patients with major depressive disorder: A grounded theory study. Psychoanalytic Psychology. Advance online publication. http://dx,doi.org/10.1037/pap00000268.
Glassman, N., & Anderson, S. (1999). Activating transference without consciousness: Using significant-other representations to go beyond subliminally given information. Journal of Personality and Social Psychology, 77, 1146-1162.
Grayer, E. D., & Sax, P. R. (1986). A model for the diagnostic and therapeutic use of countertransference. Clinical Social Work Journal, 14, 295-309.
Greenacre, P. (1954). The role of transference: Practical considerations in relation to psychoanalytic therapy. Journal of the American Psychoanalytic Association, 2, 671-684.
Greenson, R. R., & Wexler, M. (1969). The nontransference relationship in the psychoanalytic situation. International Journal of Psycho-Analysis, 50, 27-38.
Grindberg, L. (1962). On a specific aspect of countertransference due to the patients’ projective identification. International Journal of Psycho-Analysis, 43, 436-440.
Grinberg, L. 1997. Is the transference fear by the psychoanalyst? International Journal Psycho-Analysis, 78, 1-14.
Handley, N. (1995). The concept of transference: A critique. British Journal of Psychotherapy, 12(1), 49-59.
Heath, S. (1991). Dealing with the therapist’s vulnerability to depression. Jason Aronson.
Heimann, P. (1950). On countertransference. International Journal of Psycho-Analysis, 31, 81-84.
Heimann, P. (1960). Countertransference. British Journal of Medical Psychology, 33, 9-15.
Hennissen, V.; Meganck, R.; Van Nieuwenhove, K.; Norman, J.; Loeys, T., & Desmet, M. (2019). Therapists’ responses toward dependent (anaclitic) and self-critical (introjective) depressed outpatients: A multilevel approach. Psychotherapy, 1-12.
Herron, W. G., & Rouslin, S. (1982). Issues in psychotherapy. Orgin.
Hinshelwood, R. (1999). Countertransference. International Journal of Psycho-Analysis, 80, 797-818.
Hoglend, P. (1993). Transference interpretations and long-term change after dynamic psychotherapy of brief to moderate length. American Journal of Psychotherapy, 47, 494-507.
Hoglend, P. (1996). Analysis of transference in patients with personality disorders. Journal of Personality Disorders, 10(2), 122-131.
Jung, C. G. (1921). Psychological types. Collected works (Vol. 20). Bollingen.
Jung, C. G. (1946). The psychology of the transference. Collected works (Vol. 16). Bollingen.
Jung, C. G. (1966). The archetypes and the collective unconscious. Collected works (Vol. 9, Pt. 1). Bollingen.
Jung, C. G. (1969). The psychology of transference. Bolingen.
Kalsched, D. (1996). The inner world of trauma: Archetypal defenses of the personal spirit. Routledge.
Kernberg, O. F. (1987). An ego psychology-object relations theory approach to the transference. Psychoanalytic Quarterly, 56, 97-221.
Kernberg, O. F. (1994). Love in the analytic setting. Journal of the American Analytic Association, 42, 1137-57.
Kernberg, O. W. (1975). Borderline conditions and pathological narcissism.Jason Aronson.
Kiesler, D. J. (1982b). Confronting the client-therapist relationship in psychotherapy. In J.C. Anchin & D. J. Kiesler (Eds.), Handbook of interpersonal psychotherapy (pp. 280-295). Pergamon Press.
Klein, M. (1946). Notes on some schizoid mechanisms. International Journal of Psycho-Analysis, 27, 99-110.
Klein, M. (1952). The origins of transference. International Journal of Psycho-Analysis, 33, 433-438.
Klein, M. (1957). Envy and gratitude. Tavistock.
Kline, K., Hill, C., Lu, Y., & Gelso, C. (2023). Transference and client attachment to therapist in psychodynamic psychotherapy. Psychotherapy. Advance online publication. https://doi.org/10.1037/pst0000492.
Kupfer, D. J. et al. (2013). Diagnostic and statistical manual of mental disorders: Fifth Edition. American Psychiatric Publishing.
Lacan, J. (1966). Ecrits. Paris: 1966.
Lear, J. (1993). An interpretation of transference. International Journal of Psycho-Analysis, 74, 739-755.
LeDoux, J. (1995). Emotion: Clues from the brain. Annual Review of Psychoanalysis, 46, 209-235.
LeDoux, J. (1998). The emotional brain: The mysterious underpinnings of emotion. Simon & Schuster.
LeDoux, J. (2002). Synaptic self: How our brains become who we are. Viking.
Levin, F. (1997). Integrating some mind and brain views of transference: The phenomena. Journal of the American Psychoanalytic Association, 45, 1121-1151.
Levy, K., & Scala, J. (2012). Transference-focused psychotherapies. Psychotherapy, 45, 391-403.
Little, M. (1951). Countertransference and the patient's response to it. International Journal of Psycho-Analysis, 32, 32-40.
Louw, F. (2023). Klein, Kleinians, and post-Kleinians: Deeper layers of the mind and projective identification. In B. Huppertz (Ed.).Underlying assumptions in psychoanalytic schools: A comparative perspective (pp. 35-44). Routledge.
Luborsky, L. (1984). Principles of psychoanalytic psychotherapy: A manual for supportive-expressive treatment. Basic Books.
Macalpine, I. (1959). The development of the transference. Psychoanalytic Quarterly, 19, 501-539.
MacLean, P. D. (1990). The triune brain in evolution: Role in palaeocerebral functions. Plenum Press.
Malan, D. H. (1976a). The frontier of brief psychotherapy. Plenum Press.
Malan, D. H. (1976b). Toward the validation of dynamic psychodynamic psychotherapy. Plenum Press.
Mandal, M. K., & Ambady, N. (2004). Laterality and universality of facial expressions of emotions: The interface. Behavioural Neurology, 15, 23-34.
Mann, D. (1973). Time-limited psychotherapy. Harvard University Press.
Mann, D. (1999). Clinical practice in psychotherapy. In D. Mann (Ed.), Erotic transference and countertransference (pp. 1-25). Routledge.
Marmar, C. R., Gaston, L., & Thompson, L. W. (1989). Alliance and outcome in late life depression. Journal of Nervous Mental Disease, 177, 464-472.
Marmor, J. (1989). The future of dynamic psychotherapy. International Journal of Short-Term Psychotherapy, 4(4), 259-284.
Maroda, K. (1995). Projective identification and countertransference interventions: Since feeling is first. Psychoanalytic Review, 82(2), 229-247.
McDougall, J. (1978). Primitive communication and the use of countertransference. Contemporary Psychoanalysis, 14, 173-209.
Meares, R., Stevenson, J., & Comerford, A. (2005). Distinct pattern of P3a event and related in borderline personality disorders. NeuroReport, 16, 289-293.
Meissner, W. (1996). The therapeutic alliance. Yale University Press.
Mitchell, K. (2023). The importance of engaging emotions: A theological reflection (pp. 89-104). In Trist, R. (Ed). Ministry in context: A guide to theological field educator and ministry in Australia and New Zealand. Wipf & Stock Publishers.
Modell, A. H. (1980). Affects and their non-communication. International Journal of Psycho-Analysis, 61, 259-267.
Money-Kyrle, R. (1956). Normal counter-transference and some of its deviations. In D. Meltzer & E. O’Shaughnessey (Eds.), The collected papers of Roger Money-Kyrle (pp. 330-342). Clunie Press.
Nunberg, H. (1951). Transference and reality. International Journal of Psycho-Analysis, 32, 1-9. O’Crowley, A. M. (1999). The analysis of the transference: Interpretation and changes in psychotherapy. Dissertation Abstracts International: Section B: the Sciences & Engineering, 60(4-B), 1866.
Ogden, T. H. (1982). Projective identification and psychotherapeutic technique. Jason Aronson.
Ogden, T. H. (1994). The concept of interpretive action. Psychoanalytic Quarterly, 63 (2), 219-245.
Ogle, C., Rubin, D., & Siegler, I. (2012). The impact of the developmental timing of trauma exposure on PTSD symptoms and psychosocial functioning among older adults. Developmental Psychology, 49, 2191-2200.
Olnick, S. (1969). On empathy and regression in the service of the other. British Journal of Medical Psychology, 42, 41-49.
Pally, R. (2001). A primary role for nonverbal communication in psychoanalysis. Psychoanalytic Inquiry, 21, 71-94.
Perna, P. A. (1997). Reflections on the therapeutic system as seen from the science of chaos and Complexity: Implications for research and treatment. In F. Masterpasqua & P. A. Perna (Eds.), The psychological meaning of chaos: Translating theory into practice (pp. 253-272). American Psychological Association.
Pick, I. B. (1997). Working through in the countertransference. In R. Schafer (Ed.), The contemporary Kleinians of London (pp. 348-367). International University Press.
Pierro, A., & Kruglanski, A. (2001). “Seizing and freezing” on a significant-person schema: Need for closure and the transference effect in social judgment. Personality and Social Psychology Bulletin, 34, 1492-1503.
Plakun, E. M. (1998). Enactments and the treatment of abuse survivors. Harvard Review of Psychiatry, 5, 318-325.
Racker, H. (1968). Transference and countertransference. International Universities Press.
Racker, H. (1972). The meanings and uses of countertransference. Psychoanalytic Quarterly, 41, 487-506.
Rank, O., & Ferenczi, S. (1925). The development of psychoanalysis (C. Newton, Trans.). Nervous and Mental Diseases Publishing Company.
Reik, T. (1937). Surprise and the psychoanalyst. E.P. Dutton.
Renik, O. 1990. The concept of a transference neurosis and psychoanalytic methodology. International Journal of Psycho-Analysis, 71, 197-204.
Rioch, J. M. (1943). The transference phenomenon in psychoanalytic therapy. Psychiatry, 6, 147-156.
Robins, S. (2023). Understanding transference and countertransference in the direct support professions. International Journal for Direct Support Professionals, 12, 1-5.
Sandler, J. (1976). Countertransference and role responsiveness. International Review of Psychoanalysis, 3, 43-47.
Schafer, R. (1959). Generative empathy in the treatment situation. Psychoanalytic Quarterly, 28, 342-373.
Schafer, R. (1968). Aspects of internalization. International Universities Press.
Schafer, R. (1977). The interpretation of transference and the conditions for loving. Journal of the American Psychoanalytic Association, 25, 335-362.
Schafer, R. (1997). Vicissitudes of remembering in the countertransference: Fervent failure, colonization and remembering otherwise. International Journal of Psycho-Analysis, 78, 1151-1163.
Schore, A. N. (2003a). Affect dysregulation and disorders of the self. W.W. Norton & Company.
Schore, A. N. (2003b). Affect regulation and the repair of the self. W.W. Norton & Company.
Schore, A. N. (2011). The right brain implicit self lies at the core of psychoanalysis. Psychoanalytic Dialogues, 21, 75-100.
Schore, A. (2021). Right brain-to-right brain psychotherapy: Recent clinical and scientific advances. Journal of Symbols & Sandplay, 12, 1-12.
Searles, H. (1975). The patient as therapist to his analyst/Nontransference. In P. Giovacchini (Ed.), Tactics and techniques in psychoanalytic therapy: Countertransference (Vol. II, pp. 95-151). Jason Aronson.
Sharpe, E. (1930). The technique of psychoanalysis. International Journal of Psycho-Analysis, 2, 361-386.
Sifneos, P. E. (1979). Short term dynamic psychotherapy: Evaluation and technique (2nd ed.). Plenum Press.
Smith, H. (1990). Cues: The perceptual edge of the transference. International Journal of Psycho-Analysis, 71, 219-228.
Stamm, B. (1995). Secondary traumatic stress: Self-care issues for clinicians. In Researchers and Educators. The Sidran Press.
Stark, M. (1994). Primer on working with resistance. Jason Aronson.
Stein, M. (1981). The unobjectionable part of the transference. Journal of the American Psychoanalytic Association, 29, 869-891.
Stein, G. S. (1993). A transference psychosis. Journal of Clinical Psychoanalysis, 2, 345-262.
Sternberg, W. F., Bailin, D., Grant, M., & Gracely, R.H. (1998). Competition alters the perception of noxious stimuli in male and female athletes. Pain, 76, 231-238.
Stolorow, R. D. (1993). An intersubjective view of the therapeutic process. Bulletin of Menninger Clinic, 57, 450-457.
Strachey, J. (1934, 1969). The nature of the therapeutic action of psychoanalysis. International Journal of Psycho-Analysis, 50, 275-291.
Tower, L. E. (1956). Countertransference Journal of the American Psychoanalytic Association, 4, 224-255
Tummala-Narra, P. (2019). The fear of immigrants. Psychoanalytic Psychology. http://dx.doi.org/10/1037/pap0080245.
Ulanov, A. (1984). Transference/countertransference: A Jungian perspective. In M. Stein (Ed.), Jungian analysis (pp. 68-86). Northwestern University Press.
Vanaerschot, G. (1997). Empathic resonance as a source of experience-enhancing interventions. In A. C. Bohart & L. Greenberg (Eds.), Empathy reconsidered: New directions in psychotherapy (pp. 141-165). American Psychological Association.
Volkan, V. (1995) Six steps in the treatment of borderline personality organization. Jason Aronson, Inc.
Weiss, J. (1993). How psychotherapy works. Guilford Press.
Weiss. J. (1993). Patients’ unconscious plans for solving their problems. Psychoanalytic Dialogues, 8, 411-428.
Wells, J., & Wrye, H. (1991). The maternal erotic countertransference. International Journal of Psycho-Analysis, 72, 93-106.
Westen, D. (1988). Transference and information processing. Clinical Psychology Review, 8, 161-179.
Westen, D. (1998). The scientific legacy of Sigmund Freud: Toward a psychodynamically informed psychological science. Psychological Bulletin, 124, 333-371.
Wilson, A., & Weinstein, L. (1996). The transference and the zone of proximal development. Journal of the American Psychoanalytic Association, 44, 167-200.
Winnicott, D. W. (1949). Hate in the counter-transference. In Collected papers. Tavistock.
Winnicott, D. W. (1965). Primary maternal preoccupation. In J. D. Sutherland (Ed.), Through pediatrics to psychoanalysis (pp. 300-305). Hogarth [The International Psycho-Analytical Library].
Winnicott, D. W. (1988). Human nature. Free Association Press.
Wolstein, B. (1996). The analysis of transference as an interpersonal process. American Journal of Psychotherapy, 50, 499-509.


 ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com, provider #1107, is approved as an ACE provider to offer social work continuing education by the Association of Social Work Boards (ASWB) Approved Continuing Education (ACE) program. Regulatory boards are the final authority on courses accepted for continuing education credit. ACE provider approval period: 3/9/2005-3/9/2027.
ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com, provider #1107, is approved as an ACE provider to offer social work continuing education by the Association of Social Work Boards (ASWB) Approved Continuing Education (ACE) program. Regulatory boards are the final authority on courses accepted for continuing education credit. ACE provider approval period: 3/9/2005-3/9/2027. ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com has been approved by NBCC as an Approved Continuing Education Provider, ACEP No. 6323. Programs that do not qualify for NBCC credit are clearly identified. ContinuingEdCourses.Net is solely responsible for all aspects of the programs.
ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com has been approved by NBCC as an Approved Continuing Education Provider, ACEP No. 6323. Programs that do not qualify for NBCC credit are clearly identified. ContinuingEdCourses.Net is solely responsible for all aspects of the programs. ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com is recognized by the New York State Education Department's State Board for Social Work (NYSED-SW) as an approved provider of continuing education for licensed social workers #SW-0561.
ContinuingEdCourses.Net dba SocialWorkCoursesOnline.com is recognized by the New York State Education Department's State Board for Social Work (NYSED-SW) as an approved provider of continuing education for licensed social workers #SW-0561.